Volume 11, No. 2, Art. 12 – May 2010
Forming Ideal Types by Understanding: The Psychoanalytic Treatment of Suicidal Men
Reinhard Lindner & Stephen Briggs
Abstract: This paper discusses the application of a qualitative methodology—forming ideal types by understanding—to the psychoanalytic psychotherapy of suicidal men. The paper focuses on a particular phase of the methodology: the validation through external expert replication. Data of cases from psychoanalytic treatment, analysed by the originating group in Germany, is analysed by a group in London, UK, which formed to undertake the task of blind comparison. We describe the contribution of this method in the field of psychoanalytic research, the method developed for generating data and the processes through which data are analysed. We demonstrate the comparative findings from the first (German) and second (UK) analyses and explore the meanings of the similarities and differences. The paper concludes with an appraisal of the strengths and limitations (in terms) of moderate levels of generalisation of results from this method for research in the field of qualitative psychotherapy research.
Key words: suicide; suicidal men; psychoanalysis; psychoanalytic psychotherapy; ideal types
Table of Contents
1. Qualitative Research in Psychoanalysis
2. Psychotherapy and Suicidality
3. Methodology
3.1 Brief overview of the methodological procedure
3.2 Prior expectations of the two groups' assessments of the material
3.3 General methodological considerations on ideal type formation
3.4 First process of forming types by understanding (Hamburg)
3.5 The second process of forming types by understanding (London)
3.6 Sample: 20 case reports of suicidal men
3.7 The two groups of psychodynamic researchers
4. Results
4.1 Results of the first process of forming ideal types of suicidal men
4.2 Results from the second process of forming types of suicidal men
4.3 Comparison of both sets of ideal types: Similarities and differences
5. Discussion
Appendix 1: Case H, born 1958, 39 years, therapist LQ
Appendix 3: London Research: Notes from the Process
1. Qualitative Research in Psychoanalysis
There exists an ongoing debate in psychoanalysis about which philosophy of science has the most authority to lead psychoanalytical research. To simplify the many different views emerging as part of this debate, we can establish three different positions: [1]
Firstly, a "classical" hermeneutical epistemology, from which psychoanalytical findings can only be gained by genuine psychoanalytical means in the consulting room. The psychoanalyst "finds" words and actions in the patient in therapy to construct the "truth", "reconstructs" the causal conditions and gives genetic interpretations. Only observable facts emanating from the consulting room, as distinct from those taking place in the public sphere are of any importance (cf. LORENZER, 1973/2000). Such a position is, in its extreme interpretation, not very common today. Rather, some psychoanalysts (cf. PERRON, 1999, 2002; GREEN, 2000; WOLFF, 1996; ROSENKÖTTER, 1969) claim that research in psychoanalysis should reside solely in the hands of psychoanalysts in examining classical psychoanalyses. [2]
On the other side, another position emerged in psychoanalysis in the last 15 years, where psychoanalytic research has aspired to attain a "hard science" status with an empirical experimental and neurobiological epistemology (FONAGY, 1996, 1999; EMDE & FONAGY, 1997; KANDEL, 1998). In contrast to the widespread opinion that psychic phenomena are determined by multiple factors, a clarification of definitions and concepts is necessary. In this positivistic approach, objectivity matters most (HOBSON, PATRICK & VALENTINE, 1998) and measures of validity and reliability aim to provide standards of good scientific practice; "understanding" and "interpretation" need to be proved by replications. Scientists who follow positivistic scientific axioms remain sceptical toward inductive generalisation from single cases, causing single or comparative case studies to be criticised for their lack of scientific rigour (MEYER, 1993; FONAGY, 1999; WALLERSTEIN & SAMPSON, 1997). [3]
In recent years, a third epistemological position has gained increasing currency. This approach defines psychoanalysis as a "moderate hermeneutical science" (HAGEL, 1995; BOUCHARD, 1995; LEUZINGER-BOHLEBER 1995, 2002), which demands research with genuine psychoanalytical means and tools as well as systematic research strategies in order to enrich the object of psychoanalytical interest and study. These observations are validated by credibility, reflexivity and transferability. The third approach differs from the classical psychoanalytic case report in that the material leads to a new understanding (MEYER, 1993; FONAGY, 1999). It uses the psychoanalytic paradigm, always to question theoretical preconceptions and be open for the new and unknown in every case. This methodological approach is applied for example, in the study of long term effects in psychoanalyses and psychoanalytical psychotherapies of the German Psychoanalytical Association (DPV) (LEUZINGER-BOHLEBER, RÜGER, STUHR & BEUTEL, 2002). One method, basing on this approach is the method of forming types by understanding, which we will illustrate. [4]
MALTERUD (2001a, 2001b) claimed that different criteria from those established for assessing scientific rigour in quantitative research apply to qualitative studies. She suggests, as do others, that alternative criteria such as credibility, confirmability and transferability are more suitable1). MALTERUD also claims that no study achieves universal transferability. Good qualitative study designs should show a thorough consideration of what an adequate degree of transferability would consist of by presenting relevant sampling and, through "external validation", ascertaining whether or not the study hypothesis or results can be applied in other settings. [5]
As is the case with many qualitative research methods, in the method of forming types by understanding, the notion of the objectivity and independence of the researcher is abandoned in favour of recognising the impact of the researcher's direct involvement in the research process. This involvement has to be reflected explicitly and carefully to recognise preconceptions, theoretical backgrounds and work situations. When researchers work as part of a group, the interactions and dynamics of the group also need to be subject to reflexive scrutiny. Instead of the quantitative concept of reliability, in this method the primary concern is to establish credibility, i.e., the way data has to be collected in the same time period (synchronic credibility) and the method for collecting data need to be made explicit (transparency) (MALTERUD, 2001). [6]
Thus the aim of "understanding" has a central place for subjectivity, and the systematic scrutiny of subjective experiences enables the researcher to objectively comprehend, for example, psychic phenomena (RATNER, 2002). Validity in qualitative research is defined as procedural validity through transparency of the whole research process and communicative validity, i.e. triangulation through presenting parts of material or early findings to experts, external to the entire researcher or research group (STUHR, 1997). The concept of generalisability is replaced by examination of the extent and limitations of transferability. In the framework of "multiple operationalism" (WEBB, CAMPBELL, SCHWARTZ & SECHREST, 1975), transparency is gained through sample definition, and triangulation, i.e., the use of different and concurrent methods for obtaining data. Triangulation benefits and and reflects subjectivity as it furthers perception and complexity (FICHTEN & DREIER, 2003). MALTERUD (2001) claims that no study is universally transferable, but that a qualitative study design should demonstrate a thorough consideration of what an adequate degree of transferability would consist of. This can be achieved by presenting relevant sampling, whilst the transferability of findings to other settings is assessed through "external validation" (MAYRING, 2007). [7]
The study discussed in this paper is an external validation study, which goes beyond common expert supervisions during the process of qualitative research. It aims to validate an intensive expert discussion process of psychotherapy cases by the experiment of replicating exactly the processes for analysing the data by another group of experts. Experts are defined as those with knowledge and training in the field of psychoanalytic therapy. This study aims to address transferability through a systematic clinical psychoanalytical qualitative study. It will examine the qualities of "transferability" in this specific study and how this differs from "replicability" in the way this last term is used in quantitative studies. [8]
2. Psychotherapy and Suicidality
The following section introduces the psychoanalytic understanding of a specific phenomenon in psychiatry and psychotherapy: suicidality. The term is not as common in English as it is in German. It means, on the one hand, "suicidal behaviour", and on the other, "suicidal ideation". This term refers to cognitions that can vary from fleeting thoughts that life is not worth living, via very concrete, well-thought-through plans for killing oneself to an intense delusional preoccupation with self-destruction (DIEKSTRA & GARNEFSKY, 1995). Suicidality encompasses the whole spectrum of thoughts, expressions and actions concerning suicide, including all thoughts from ideas that life is not worth living to concrete, well-structured plans how to kill oneself up to the paranoid commitment to self-destruction (CHILES & STROSAHL, 1995). [9]
Several technical terms are briefly introduced to understand the psychoanalytic theories of suicidality. First, "transference" refers to a psychological process in which unconscious wishes directed toward past relationships, especially those originating in childhood, are reactivated in a present relationship (LAPLANCHE & PONTALIS, 1972). "Counter-transference" is the specific reaction in the psychotherapist, triggered by the patients transference but mixed up with the own unconscious internal world of the psychotherapist and his or her own early wishes toward the parents. Transference includes the ubiquitous process of "projection", where a person locates his or her wishes, affects or behaviour in another person (LAPLANCHE & PONTALIS, 1972). [10]
Following FREUD's (1917) formulations, psychoanalysis has developed a distinctive theoretical framework for understanding suicide which is primarily relational:
"Suicide is an act with a meaning and a purpose, both manifest and unconscious. It takes place in the context of a dyadic relationship, or rather its failure, and the suffering is experienced by the survivors, or rather, part survivors, of the suicide attempt" (HALE, 2008, p.19). [11]
In psychoanalytic treatment of suicidal people, the central preoccupation is how relatedness is experienced in the therapeutic relationship in the transference and counter transference. This is seen as a very challenging situation because the nature of suicidality is such that it can escape conscious recognition, observation and direct exploration, as the purpose and meaning of suicide lies outside the patient's consciousness. On the other hand, relationships with suicidal patients are often strongly defined by negative emotional reactions, experiences which are understood to stem from and reflect the hostility and violence of suicide, aggression turned against the self, and the projection of these into the therapist who can, unwittingly, be pushed into playing the role of an "executioner" if (s)he does not intervene, or responds inadequately to prevent the suicidal impulse (CAMPBELL, 2008; MALTSBERGER & BUIE, 1974). [12]
The elusive character of suicidality and the presence of negative emotional reactions (transference and counter transference) contribute to difficult and often anxious therapeutic environments. Anxiety is particularly enhanced at the beginning of the therapeutic relationship with suicidal patients as the consequences are potentially fatal. It is therefore of significant importance in the diagnosis and therapy of suicidality that the therapist is flexible in dealing with initial contacts and relationships. The therapist needs to be able to communicate understanding empathically to the patient, and to use the counter-transference experiences to the benefit of the patient. [13]
The concept of the "triangle of understanding" (MENNINGER & HOLZMAN, 1977; MALAN, 1979) was developed to explain the process of therapeutic relatedness with patients in psychoanalysis. Congruent relationship patterns were studied to achieve flexible and congruent understanding in three domains: first, the transference situation in the therapy session; second, in the reality of the actual (suicidal) life situation as described by the patient to the therapist; and third, in the childhood situation learned from the patient's biography. In suicidal patients this psychoanalytically orientated diagnosis permits both a perception of important signals of the actual danger of suicide, as well as an understanding of its biographical significance (GERISCH et al., 2000). To understand a patient through all three dimensions requires the therapist to develop a strong therapeutic relationship with the patient (LINDNER & GERISCH, 1997; FIEDLER & LINDNER, 1999; GERISCH et al., 2000). [14]
Gender difference is obvious in suicide. In western countries, men commit suicide more frequently than women; however, women attempt suicide more frequently than men (HAWTON, ZAHL & WEATHERALL, 2003). There are differences in suicide strategies/means resorted to by men and by women, and intrapsychic dynamics may also be different. Therefore, exploring suicidal dynamics should include a gender-sensitive approach. So far, psychoanalytical patterns of explanation for suicidality have only sporadically looked at differentiated gender aspects of suicidality (e.g. GERISCH, 1993, 1998, 2003). In this research project, we study only one gender: men. Specific areas of disturbance among suicidal men arguably correspond with childhood development, and especially with disturbance during the early experience of relatedness to the mother, with specific conflicts in the developmental area of separation and individuation as defined by MAHLER, PINE and BERGMAN (1975), and with failed experiences of relating to a "third" person, like a father. In contrast with men, women seem to be more prone to committing suicide when their introjection of the devalued mother combines with a partial identification of an idealised father. This leads, in relational conflicts, to reactions such as masochistic clinging to a destructive relationship. One cause of this gender difference may be that girls/women may be confronted with the issue of feeling different from their mothers, rather than sharing physical similarities with her but boys/men may have problems in feeling bound to their mother, father or any other important object from early childhood (GERISCH, 1996, 1999). These theoretical assumptions are supported by empirical studies: they show the significant connection between psychic abuse, sexual abuse, neglect, rejection and loss experiences with subsequent mental illnesses and suicidality (BREWIN, ANDREWS & GOTLIB, 1993; HARKNESS & MONROE, 2002). In addition, suicidal men tend to have more problems with substance abuse and real as well as fantasised violence, which can be seen as an expression of problems in experiencing separation without being overwhelmed by destructive impulses (HERZOG, 1980, 1982). [15]
The manner and expression of these patterns of relatedness mostly indicate aspects of disturbance in core relationships during early childhood. Additionally, biographical factors leading to suicidality tend to occur during a development period from which clear memories barely existed; but they can be revealed in psychotherapy in the way the patient adopts and forms the therapeutic relationship (FREUD, 1914; DENEKE, 1993; FONAGY, 1999). The patient's biographical descriptions should be understood, particularly in the critical-suicidal state at the beginning of psychotherapy, as part of the events belonging to a current re-enactment of early childhood relationship patterns. Therapists' understanding of events often become evident through the patient's response to the therapist's attitude or holding function which acts as a support to maintain and enhance the observing, anxiety-containing, and integrative capacity of the patient (WINNICOTT, 1965). Interpretations are given only later (DENEKE, 1993). [16]
Suicidality is therefore a complex, acute, occasionally latent and quite frequently unconscious phenomenon determined by multiple factors. The methods for recording suicidality in a clinical framework must take this complexity into consideration. Thus the aim of studying patterns of relationships for suicidal men in psychoanalytic treatment should be to include assessments of all three dimensions of the "triangle of understanding" in order to explicate the particular qualities of each of the three dimensions of this triangle:
transference-counter transference (i.e. what happens between the patient and the psychotherapist in psychotherapy and how to understand it),
current relationships and (psychopathological) symptoms and
past (childhood) relationships, biography and important life events. [17]
3.1 Brief overview of the methodological procedure
In this study, two independent groups of psychodynamic researchers went through a discussion phase to understand the complex interactions between biography, therapeutic relationship and suicidality of 20 suicidal men, coming into psychodynamic psychotherapy. The first group of psychodynamic researchers included the respective psychotherapists of the patients and is a group of experienced clinical psychotherapists/psychoanalysts and researchers at the Center for Therapy and Studies of Suicidal Behaviour in Hamburg. The other group operates at the Tavistock Clinic in London, and is composed of psychodynamic psychotherapists. Both groups developed ideal types of suicidal men at the beginning of the psychotherapy. The method and its application in this study are described below. [18]
3.2 Prior expectations of the two groups' assessments of the material
Before the research was started, we had some ideas about how and why the two groups might reach different and similar conclusions. It was obvious that the two groups differed in important ways and it was reasonable to expect that this would lead to differences in the process and outcome of the research. These differences included:
In the group based in Hamburg, Germany, each therapist took part in the discussion and was able to give additional information on his/her respective case at different stages of the process. The members of the UK-based group had to ground their judgements solely on the written case material, because the patients' psychotherapists, who could deliver more information, were only present in the first group.
Both groups had access to identical written materials, including recordings of the research group supervision for each case study conducted in Hamburg.
Although the members of both groups had a psychoanalytical background, they might favour different theoretical schools, have different clinical experiences and different cultural backgrounds. [19]
We anticipated that there might be some similarities in the results, stemming from the psychoanalytical assumptions shared by both groups as well as from a common understanding of therapeutic work with suicidal patients. Such findings, based on similarities, lead to the formulation of another level of ideal types characterised by a higher degree of transferability. [20]
3.3 General methodological considerations on ideal type formation
The need to proceed systematically (i.e., to deliver understandable and verifiable results and to bring them to a more general level) conflicts, to some extent, with the need to ensure that the data is not isolated prematurely and distorted by abstraction (STUHR, 2001). Any prejudiced opinions, theoretical concepts and personal attitudes on the part of the researcher must be taken into account, named whenever possible and described a priori (GERHARDT, 1999). A qualitative method that aims to generate new hypotheses, rather than merely confirming old ones, must be open to the clinical-therapeutic creativity that a psychotherapist needs to understand the individuality of his/her patients, respect it and, at the same time, integrate it into the general picture. [21]
The method of forming types by understanding is suited to this approach. It is a systematic, qualitative method, originating from qualitative social research (GERHARDT, 1990, 1991, 1994a, b, 2001; KLUGE, 1999, 2000; KELLE & KLUGE, 1999; FROMMER, LANGENBACH & STREECK, 2004). Its basis is the theoretical construction of ideal types. According to Max WEBER, the ideal type has "the importance of a pure borderline term ... against which reality can be tested to clarify certain significant parts of its empiric content, with which it can be compared" (WEBER, 1904/1988, p.194; GERHARDT, 1999). In psychoanalytic psychotherapy research, forming types by understanding systematically resorts to genuine psychoanalytical methods of acquiring knowledge: initial interview techniques, scenic understanding (KLÜWER, 2001), case reports, supervisory case research seminars, and triangulation of qualitatively acquired knowledge with results from accompanying quantitative surveys (WACHHOLZ & STUHR, 1999; STUHR & WACHHOLZ, 2001). It occupies a hinge-like position, between exemplifying single case studies and operationalised measurement through analysis of data from large samples. From this position it spearheads the direction of research into psychoanalysis, psychotherapy, psychiatry and medicine. This is especially true when the object of research, such as subjective human relationships, is clinically relevant, but resists direct measurement and observation (HEMPEL, 1965: SCHWARTZ & WIGGINS, 1987a, b; MALTERUD, 2001). The methodology is therefore likely to achieve a higher degree of credibility, dependability, confirmability and transferability than single case studies while also retaining greater correspondence with practice, and hence to be endowed with more authenticity than more practice-distant positivistic methods. [22]
Using this methodology, our objectives for the study were twofold: first, we expected to gain transferable and more generalisable results concerning the transference/counter-transference situations and biographical features in the beginning of the psychodynamic psychotherapy with suicidal patients. Second, we expected to gain more information about the transferability of results through the method of forming types by understanding. In terms of methodology more broadly speaking, we hope to contribute to the development of standards for systematic qualitative research in psychoanalysis. [23]
3.4 First process of forming types by understanding (Hamburg)
The process of forming types by understanding will be illustrated through our example of psychotherapy with suicidal men. The process makes use of psychoanalytical methods, and also employs systematic qualitative methods stemming from social research. These include case contrasting and confrontation and systematic development of ideal types (WEBER, 1904/1988; GERHARDT, 1990, 1994a, b). The practicability of the method has been demonstrated in several studies (STUHR, 2001; STUHR & WACHHOLZ, 2001; STUHR et al., 2001; STUHR, HÖPPNER-DEYMANN & OPPERMANN, 2002; LINDNER, 2003). Here we will describe the processes used in our study. [24]
3.4.1 Case reconstruction
After a minimum of the first five sessions of psychotherapy, therapists write a case report about the three aspects (biography, suicidality and transference/counter-transference relationship). The case is presented and discussed in a supervisory research seminar, and from this a full case report is written. (As an example a full case report is included in Appendix 1.) [25]
3.4.2 Case contrasting
A group discussion of each case takes place to address the research questions, developed from the "triangle of understanding":
Which biographies lead to which kind of suicidality?
Which biographies lead to which transference/counter-transference situations in the first five sessions?
Which transference relationship is an expression of which form of suicidality? [26]
In repeated iteration, through moving between discussion of case material and general themes or "aspects" from the material, clusters of similar cases are put together in a group discussion. A single prototypical case for each cluster is selected by choosing the one case which best represents the cluster. Protocols are developed from these case discussions. [27]
The group discussions function as a "negotiation model", as WESTMEYER (1979) formulated it. Members of the group can be thought of as taking up involuntary roles, such as "the practitioner", "the reality prover" (the person in the group who questions the arguments and interpretations critically), "the expert" or "the methodologist" to keep the group process moving. In a way, these case discussions are a form of group discussion, as in social sciences (BOHNSACK, 2000; DREHER & DREHER, 1995; STUHR, 1995). [28]
The protocols of both case discussion processes for Hamburg (in German) and for London (in English) are attached in the Appendices 2 and 3. [29]
3.4.3 Case confrontation with prototypes ("sighting-disc-rating")
The "sighting-disc-rating" was initially developed for the method of forming types by understanding (STUHR et al., 2002). The rating offers a possibility to gain measurable data on similarities and differences between each single case and each prototype. [30]
The prototypes are placed on the outer circle of a sighting-disc and each individual case in the centre. Each research group participant determines the proximity of each specific individual case to each of the prototypes by means of tangents. Discussion continues until unanimous agreement on the tangents is reached. [31]
3.4.4 Structural analysis and forming of ideal types
The "sighting-disc-rating" facilitates description of the similarity or difference of each single case to each prototype. This allows the "storage" of similar types of cases. The cases that are repeatedly and unanimously assessed as being similar in a specific aspect are grouped together. Going back to the case material, the common aspects developed in the case-contrasting process are described—again at a meta-psychological level—as ideal types. After this, in a more generalising effort, each case is assigned to the ideal type, which is most characteristic of the case. Then, different hypotheses are tested to give more context and explanation to each ideal type; through consideration of the case material assigned to each ideal type, several hypotheses are tested, namely the distribution of socioeconomic variables (age, profession), the previous psychiatric and psychotherapeutic treatments and the duration of the actual treatments, the severity of suicidality and aggressive behaviour in each ideal type, the gender matching distribution (patient: male/female therapist), the distribution of biographical specifics (e.g. the presentation of relationship to primal objects, early traumas, use of alcohol and other drugs, representation of the body. [32]
3.5 The second process of forming types by understanding (London)
The process for comparison by the London-based group included translation into English of the "case book" composed of 20 cases of suicidal men seen in TZS. The four raters based in the Tavistock's Adolescent Department formed a research group and the group took part in a workshop on "forming types by understanding", where the method, the clinical situation of the patients and the general psychotherapeutic orientation of TZS were explained. The results of the study were not revealed to ensure that the group remained blind to the earlier study and its outcomes. Each participant in the Tavistock research discussion group read the case book, and the group met for three consecutive days for a total of 21 hours to discuss the cases, starting with individual case discussion, and moving on to comparing cases and developing more general themes. The group wrote down the essential characteristics of each of the three aspects (biography, life situation, transference/counter-transference), to identify one case (prototype), which best represents this aspect. In these 4.5 hours of discussion the group undertook the "sighting-disc-rating" (case comparison) for each prototype to compare each case with each prototype. The results of the sighting-disc-rating were discussed and one agreement for each comparison was defined. Finally, the results of the Tavistock group were compared with the results from the TZS group in a one-day workshop in TZS. Similarities and differences were discussed and recorded. A process note was written for the whole discussion process (see Appendix 3). [33]
3.6 Sample: 20 case reports of suicidal men
The study was carried out on a sample of the 20 most recent male patients who had had at least five psychotherapy sessions at TZS. The sample is closely representative of the generality of male patients at TZS (FIEDLER et al., 1999) in terms of age, social status and psychiatric diagnosis. Men living alone were over-represented in the sample compared to the patients at TZS. One man had a homosexual orientation (Case T), all other men were heterosexuals. All 20 patients had suicidal intentions, 12 patients had a history of suicide attempts, 11 of which occurred less than six months before the beginning of psychotherapy. Neither the therapists nor the patients knew anything about the selection of patients for a study during the first five psychotherapeutic sessions. [34]
3.7 The two groups of psychodynamic researchers
The first group: Center for Therapy and Studies of Suicidal Behaviour (TZS), University Hospital Hamburg-Eppendorf
TZS is a psychoanalytically-orientated facility with specialised out-patient treatment for seriously clinically-disturbed patients in suicidal crises within the University Hospital Hamburg-Eppendorf (TZS) (FIEDLER et al., 2007). TZS psychotherapists (N=5, plus one research psychologist) work as psychoanalysts and/or analytic psychotherapists as well as specialist psychiatrists or psychologist-psychotherapists registered as out-patient psychotherapists and officially recognised by national medical insurances. In addition to providing out-patient clinical psychiatric psychotherapy, TZS also maintains a "Suicidality and Psychotherapy" research group which is nationally and internationally active in the field of scientific study for the understanding and therapy of suicidal behaviour. Patients are referred or recommended for treatment by other physicians or psychologists, but also come of their own accord in a suicidal crisis (FIEDLER et al., 1999, 2007). [35]
The second group: Adolescent Department, Tavistock Clinic, London, UK
The Tavistock Clinic, now a Foundation Trust in the National Health Service, provides a mental health service for children and families, adolescents and adults, in which psychoanalytic psychotherapy is an important model of intervention. Additionally it is a national and international training centre, providing trainings for the mental health personnel, psychotherapy and the application of psychoanalytic thinking to a wide range of professionals. The rating of clinical texts in this study is undertaken by psychoanalytic psychotherapists, who are members of the Adolescent Department's research group. [36]
4.1 Results of the first process of forming ideal types of suicidal men
The first process (in Hamburg) of analysis of this sample and the assignation of ideal types provided a basis for the comparison. These results are briefly reproduced here (for more details see LINDNER, 2006). A total of four ideal types was developed.
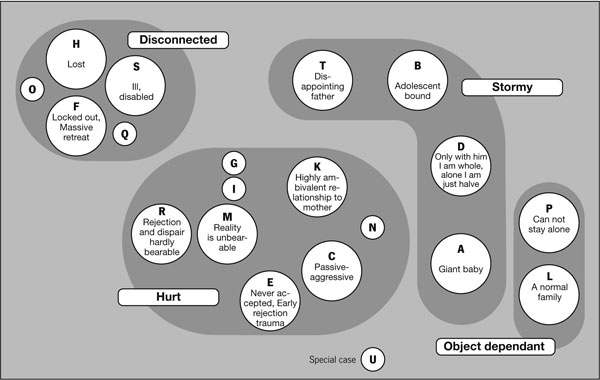
Illustration 1: The four ideal types "Disconnected", "Hurt", "Stormy" and "Object dependent" are formed out of similar prototypes
(big circles) and single cases (small circles). Similarity also occurs between different ideal types: e.g. case N is similar
to prototype K and C from ideal type "Hurt", but also to prototype D and A from ideal type "Stormy" (LINDNER, 2006). [37]
The descriptors of these four ideal types, based on biography, current life and transference/counter-transference aspects are: [38]
Ideal type A "Disconnected": In the transference/counter-transference relationship, a disconnected experience prevails between patient and therapist, providing little continuity and support for the therapeutic relationship. This feeling corresponds with the suicidal dynamics of repeated rejection experiences. The patient acts with an aggressive reproach in both in the transference and suicidal events. This can be interpreted as a re-actualisation of the conflictual experience of parental exclusion. [39]
This ideal type contains a strongly ambivalent relationship with their father, which, in the transference, determines the therapeutic relationship. Their bond with their mother, on the other hand, seems "pale" and unsubstantial. In this ideal type, patients make suicide attempts with highly lethal potential. Correspondingly, in-patient psychiatric treatment is frequent before the start of psychotherapy. At the beginning of therapy, the patients appear to be in a very bad, partly acute somatic condition. Any alcohol or cannabis consumption causes withdrawal from important relationships. [40]
Ideal Type B "Hurt": There is often an aggressive entanglement between the patient and the therapist, in which the patient, anticipating rejection, is passively or actively aggressive. Aggressive emotions predominate in the counter-transference. Similarly, suicidal dynamics are characterised by real experiences of loss, which mobilise aggression, and simultaneously (temporary) unbearable feelings of emptiness, immediate need for another person to be here and the awareness of having failed in important (relationship) goals in life. Real trauma occurs frequently in biographies, and triangulation experiences are absent. [41]
In childhood, these patients experienced themselves as self-object2) of the mother, whereas the father was mostly experienced as absent. Often a significant woman (mother, girlfriend, female therapist) recommended treatment. Both hospitalized and out-patient psychiatric-psychotherapeutic treatments are frequent. This ideal type shows evidence of chronic suicidality (although perhaps not so much as in "Stormy" and "Object Dependent" ideal types), and patients are more likely to come for treatment shortly before than after a planned or threatened suicide attempt. The men are often strongly built, sporty and well-dressed, but exude a sense of great tension. The need to conceal some physical defect, weakness, hypochondriac anxieties or insecurities is frequent. [42]
Ideal type C "Stormy": A stormy transference (e.g. patients having conflicting wishes towards the therapist) generates, surprisingly, relatively little annoyance in the therapist, and more frequently mobilises a desire to help. This is a reproduction of the comfort-searching side of a (late adolescent) separation-dependency conflict. Suicidal feelings are, therefore, connected with separation experiences, as well as with the development of a fixation on a certain psycho-social development level. Very intensive, ambivalent bonds to the mother appear in the biographies. [43]
Patients often report destructive parental relationships, that is, of fathers physically threatening the mother, as if the patients feel they had to protect their mother and her life. At the same time, identification with the violent father is highly ambivalent. Emotions are inadequately controlled. Their outward appearance is based on one-dimensional, aggressive male concepts, e.g. the hard worker or the warrior. They have a tendency to have strong outbursts of emotion. Alcohol and/or cannabis consumption reflects an unconscious surrender to a dangerous, destructive object. [44]
Ideal type D "Object dependent": In the transference relationship, there must be no "third" element, not even as an explanation for the current experience. Therefore, only concrete matters can be queried and dealt with. Accordingly, these men want the women who have turned away from them to return. The biography seems simplistic and conceals a lack of emotional experience. One has the impression that an experience of chronic emotional neglect is warded off by idealising and identifying with family norms (e.g. "solidarity" or father's occupation). [45]
Patients report supposedly pleasant childhoods, although the description seems evasive. In connection with a specific counter-transference experience (under pressure and having to make "sense" of everything alone) the impression is formed that they were emotionally neglected in childhood. Stable psycho-social arrangements can support for a long time defence against feelings and conflicts associated with the neglect. Patients only become suicidal when these relationship constellations and their inherent defence mechanisms are threatened. If alcohol is consumed in the framework of a suicidal experience, it is an unconscious cry for help to an inanimate object, which, however, provides no protection. [46]
In the sample, there is one special case (Case U) of an abused and abusing man who has little similarity with all other cases, and is marked by a specifically highly aversive counter-transference reaction. Also, another two prototypical constellations were heuristically developed that were not in the sample, which are rarely seen at the Therapy Centre: older men and patients with acute psychiatric illnesses, such as seriously depressive episodes or chronic schizophrenic psychoses. The special case and the heuristically "composed" constellations point out that there are probably further types of suicidal men who, within other cultural paradigms, and also in other clinical settings, (e.g. help lines, Samaritan counselling centres, in-patient psychiatric services) occur more frequently.
|
Type |
Cases/ |
Object Relations |
||
|
|
Prototypes |
Suicide |
Transference |
Biography |
|
Disconnected |
F, H, O, Q, S |
Experience of disconnection |
Refusal |
|
|
Hurt |
C, E, G, H, K, M, R |
Aggressive entanglement, realisation of disillusioned reality |
Aggression and refusal |
Traumatic experiences of loss |
|
Stormy |
A, B, D, T |
Separation, realisation of a fixation on a certain developmental level |
Attached-welded, mobilizing helping desires |
Unsolved dependency conflicts |
|
Object dependant |
L, P |
Separation, the woman must come back |
Concreteness3) leads to distress in therapist |
Lack of emotional containment in childhood |
|
Special case |
U |
Shame |
Seduction warded off |
Different cultural background, sexual and violent abuse |
Table 1: Results from the first discussion: There are four ideal types with the cases assigned to them, the prototypical cases are indicated. Case U is indicated as a special case, which could not be assigned to any ideal type. [47]
4.2 Results from the second process of forming types of suicidal men
The second process undertaken by the Tavistock group—blind to the findings of the TZS group—led to the formation of three ideal types: [48]
Ideal type A "Withdrawn loner": The model in literature is Monsieur Bovary (FLAUBERT) as a schizoid self-destroying man. These men present a "thin-skinned narcissism" (BRITTON, 1998) that causes every approach from the outside to be experienced as an attack. The resulting aggression must be projected into the outer world again. These men still fight, because they come into treatment in contrast to some homeless suicidal people but in the transference relationship they unconsciously, and thus actively destroy all therapeutic attempts to come into a contact with them. So the transference situation is characterised by withdrawal. The main biographical aspect is that of a loner. [49]
Ideal type B "Sado-masochistic enmeshed": These men create unpleasant relationships; in current relationships with partners or past relationships with parents they cannot separate but cannot live together either. In this ideal type there are only a few suicide attempts. These men seem to be linked to the subjects with whom they reproduce enactments of the struggles with suicide and rejection (JACOBS, 2000; KLÜWER, 2001) leading to attempts to cling to the therapist, the counter-transference is about dealing with feelings of wishing to control the patient. It was hard for the members of the discussion group to "stay in the room" with these patients, meaning that they expressed the wish not to discuss these cases any longer. In biographies there are lots of controlling and enmeshed relations with suicidal parents with mental illnesses as well as absent fathers and frightening and controlling mothers. [50]
Ideal type C "Psychotic—unrealistic": These patients resorted to "psychotic" solutions, in psychoanalytic terms: they would fall in love in order not to experience their anxiety and separateness. The lack of anxiety is the result of the defence of splitting relatedness to "good" and "bad" so that the anxiety is projected into the "bad" object and thus is experienced as not belonging to the self. The transference situation is characterised by a tendency to merge or fuse with the therapist. The biographies often reveal intense and idealised relations.
|
Type |
Cases/ |
Object relations |
||
|
|
Prototypes |
Suicidality |
Transference |
Biography |
|
Withdrawn |
E, F (regressed), H, M, O, P, Q
|
Isolated, Suicidal ideation, Masked attempts |
Withdrawn |
Loner |
|
Sado-masochistic enmeshed |
A, B, C, G, L, N, R, U
|
Few attempts, object linked
|
Cling/Control |
Controlled, Enmeshed relations |
|
Psychotic-unrealistic |
D, K, S, T
|
Psychotic solution |
Merging |
Intense idealised relations |
Table 2: Results from the second expert discussion: There are three ideal types with the cases assigned to them; the prototypical case is indicated. [51]
4.3 Comparison of both sets of ideal types: Similarities and differences
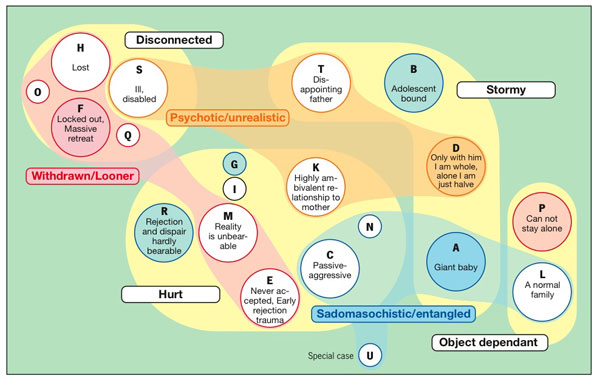
Illustration 2: The ideal types of the second formation process are projected on the ideal types of the first formation process.
Red: Ideal type "Withdrawn", yellow: "Psychotic-unrealistic", blue: "Sadomasochistic-enmeshed". [52]
Initial observations appear to show that the TZS and Tavistock groups developed different sets of ideal types, which are identified through both the different groupings of cases and the different language used to describe ideal type. The two groups were using different criteria—especially theoretical—to assess the cases, which resulted in different classifications as ideal types. This is evidenced by the fact that all three ideal types of the Tavistock group spread over three of the four ideal types of the first group. [53]
On the other hand, there are some similarities between the two research groups, which can be discerned through closer examination. For example the following groups of cases CNALU, OFQ and TKD are clustered together by both groups, meaning, that both research groups found these cases to be similar to each other. Moreover, no patient from the ideal type "Withdrawn" (London group) was placed in the ideal type "Stormy" (Hamburg group); no patient from the type "sado-masochistic enmeshed" came from the ideal type "disconnected" and no patient from "psychotic-unrealistic" came from "object dependant". This analysis leads to the hypothesis that the diagnostic assessment criteria, which generated most similarities stems from experience-based criteria, that is, from the counter transference aspect. Psychotherapists can "feel" one patient to be similar to another, but how they explain this phenomenon may be very different due to the use of different theoretical approaches. Both groups of therapists were quite similar in their assessments of aspects they could feel and experience in the therapeutic relationship out of a common clinical experience. These are experiences about the quality of the therapeutic contact, whether the patient (and the therapist) is remote and distant or whether there is an intensive, aggressive, manipulative or idealising transference situation. Another similarity in both groups seems to be the assessment of aspects of the transference relationship, for example, the discussion of illusory or unrealistic relationships or relationships in which no inner meaning can be found. It seems very likely that similarities found by both groups arise from clinical experiences of the quality of the therapeutic relationship. [54]
On the other hand, differences seem to stem from the two quite distinct theoretical approaches used by the two groups to understand the interactional patterns within the cases. It is important, therefore, and consistent with our methodological approach, to explore the nature of these differences. The TZS group of German psychoanalytic psychotherapists had their theoretical background in the work of the psychoanalyst Heinz HENSELER (1974) who influenced the psychoanalytic understanding of suicide in German psychiatry for decades with a self-psychological understanding of suicidality as a narcissistic crisis. Other concepts used in the German group came from the work of KIND (1992), who chose an object-relational framework for a clinical taxonomy, theories on adolescent autonomy-dependency conflicts (LAUFER & LAUFER, 1989) and the Kleinian work on symbolisation. [55]
The Tavistock group was influenced by a different theoretical framework, drawing on Kleinian theory as developed by subsequent theorists, particularly BION (1962, 1970), BRITTON (1989, 1998), ROSENFELD (1987) and JOSEPH (1989). This framework emphasises the elemental conflict between life and destructive forces, the projection of destructive elements into others and the impact of these on the therapeutic relationship, generating re-enactments of sado-masochistic relatedness. In suicidality, destructive narcissism is seen as a defence against the pains of the depressive position (KLEIN, 1957/1975). Additionally, the Tavistock group is influenced by developmental theories of adolescence (ANDERSON & DARTINGTON, 1998) and the Freudian idea of the core conflict, in which neither separation nor intimacy is tolerable. [56]
We embarked on this study with the hope and expectation that some (forms of) similarities across the two groups would be found, and that these would provide evidence for the transferability of findings beyond the immediate context of the study. Such transferability would provide strong evidence that the method of forming types by understanding can be used in other psychoanalytic settings to develop robust research, which is, however, practice-near (FROGGETT & BRIGGS 2009) and qualitative. At the same time, we were aware of the potential differences between the two groups of researchers, who had different national and historical backgrounds and, following from this, different heritages in terms of psychoanalytic theory and practice. The two groups also differed in their knowledge of the cases. The London/Tavistock group only had the written case book as knowledge of the cases whereas the Hamburg/TZS group had additional first-hand knowledge of the patients and the presence of the therapist in the research discussions. Given these differences we expected that the study would provide both differences and similarities that we could find and account for. [57]
Our findings show that the groups differed in the way they developed ideal types, the descriptions for these and the theoretical frameworks that drove the conceptions that formed our clustering, as described above, into different ideal types. We found that similarities existed at the level of the clinical experience. The transference/counter-transference domain was central for the appreciation of similarities. This analysis suggests some ways of analysing the data, comparing these through the clustering of similar cases and the similarities of descriptors within ideal type categories provide a starting point for developing transferability. [58]
From this study, it is suggested that the three aspects of each case—biography, current situation, transference/counter-transference—provide a solid basis for developing this kind of comparative study about an important psychosocial phenomenon like suicidality. Qualitative research does not usually focus on transferability and generalisability of results, except in the demand to work thoroughly, to give a clear description of the material, patients or persons who are investigated, and to present the material and the methodical steps so that anyone can follow the heuristic steps from the material to the concluding results. Rather, some qualitative researchers such as MAYRING (2007) claim that generalisability is very important for qualitative research to come to results that can lead to political, medical or psychotherapeutic action. [59]
In psychoanalytical discussions the question of the frame and limits of general statements are not very often discussed; theoretical considerations stemming from very different cultural and theoretical backgrounds are often presented without mentioning these limitations. Therefore it is of value to show on which level the same material can lead to different but also, on another level, similar results when examined by different experts. In a quasi experimental setting it can be shown that speaking about patients may on the one hand lead to totally different interpretations and on the other lead to similar results. The interesting finding of this study is that similarity can be achieved on the basis of the common understanding of the interaction between patient and psychotherapist, called the transference/counter-transference-relationship. [60]
From a methodological perspective, the possibility to find common interpretations can be defined as a form of "moderatum" or mid-range generalisations as defined by WILLIAMS (2006, p.138):
"[They] arise from that cultural consistency and are the basis of inductive reasoning in the lifeworld. ... Moderatum generalizations I advocate are, then, the bridge between the ideographic and nomothetic. ... They can provide testable evidence of structure and outcomes of structure. Their limits lie in the logical problem of inductive inference and in the ontological problems of categorial equivalence". [61]
WILLIAMS explicitly mentions that WEBER's ideal types are logically equivalent to theories. [62]
These results lead to the suggestion to present the clinical material in a way that the therapeutic relationship can be understood easily, that the reader is able to remember own experiences with similar patients and through this may connect with the clinical knowledge. This can be achieved by presenting the case without theoretical metapsychological considerations by just "telling the story" as DENEKE (1993) advocates. [63]
Interpretative psychoanalytic research would not aim to, and cannot achieve, (much) more than moderatum generalisability (WALKERDINE, LUCEY & MELODY, 2002). (Inter-) subjectivity is and should not be ruled out in finding an understanding of another person's inner world because the process of understanding is only possibly done through the researcher's personal and partly unconscious inner relations to the material. This being said, the finding that a thorough use of transference and counter-transference analysis produces some similarities between the two groups of researchers provides evidence for the credibility of this instrument, without stretching its meaning to the domain of impersonal "truth". [64]
Future development of the method would focus on the meaning of differences in order to both appreciate the different approaches within different national and theoretical backgrounds and to get beneath these distinctions to appreciate the clinical phenomena. As a continuative research a case report can be used to interpret an ongoing process between two groups, which always share not only their interpretations of the material but also the theoretical, personal and cultural reasons for them. This may lead to more scientific consistency in an interpretive science like psychoanalysis. [65]
The authors wants to thank Georg FIEDLER, Ilan GANS, Benigna GERISCH, Paul GÖTZE and Monika RICHTER from the Hamburg research group and Jonathan BUHAGIAR, Will CROUCH, Samantha GOTTHARD, Lydia HARTLAND-ROWE and Liz WEBB from the London research group for their intensive engagement in the research process by sharing their knowledge, creativity and libidinal cathexis to their work with suicidal patients. The English translation of the case book was performed by Sigrid WEISE.
This research was supported by a research grant from the Research Advisory Board from the International Psychoanalytic Association (IPA) and the Forschungskolleg Geriatrie of the Robert Bosch Foundation in Stuttgart.
Appendix 1: Case H, born 1958, 39 years, therapist LQ
This case report is a translation from one of the Hamburg case reports as an example of the 20 reports. The initial material stems from session protocols. The case reports were written by the therapists. Each participant in both groups had to read the case reports in advance before the case-contrasting discussions.
First five therapy sessions
Mr. H. was referred to me by the nephrology department.4) After a serious suicide attempt with a mixture of different tablets he had first been taken to the psychiatry department but then, after an acute renal failure, been transferred to the dialyses section. At the time of his first appointment Mr. H. was no longer a dialyses patient.
At the first appointment I greet a very tall, lanky 38-year-old man, visibly worn out by his ill physical condition. He attempts to be relaxed when greeting me. His depressed and resigned state of mind beneath the surface can be sensed at once. During our talks, he keeps staring into the distance. He remarks that since his suicide attempt his situation has not changed. For him the kind of life he is leading makes no sense. The acute reason for this is the separation from his girlfriend he was with for many years. She has decided to live with another man. For over six years there have been continual see-saw changes. He finds it difficult to have a close relationship with somebody, but he does long for one. In fact, his girlfriend stuck with him for quite a while. He prefers living with his half-blind sheep dog, which he "needs". In contrast, he defines his attachment to his girlfriend as a "desire" for her. It is terrible for him to realize that when he had opened up to her more than ever before, she chose another man she had known for some time already. She still takes care of his dog, and they are still in touch. He only feels fine when he is busy doing something he likes to do. Then he feels easy, acting out his abilities. He always needs a certain atmosphere, for example when he makes music, or when he thinks of the time he worked for an artist in P. He then used to work with pleasure and loved what he did. He also liked living in a motor home with his dog. On my inquiry he tells me about some events from the past years, especially about his father's death, as well as the deaths of several friends.
During our talks I have the impression that Mr. H. is not sure of himself. It becomes clear to me that the attention he received when he was under watch is exactly what he needs. Obviously he has a talent for mobilising doctors, nurses and orderlies; even the cleaning woman and surrounding patients seemed to attend to him in a touching way, as well as a woman from the social services at the University Hospital Hamburg-Eppendorf, Mrs. R. At the same time he conveys the impression that all this does not have an effect upon him; as soon as he is alone the inner emptiness comes back immediately. Soon after our first appointment Mr. H. calls me to be able to talk to me before our next session. Since it is impossible for me, we meet again only one week later at the fixed date. Right from the beginning he says he regrets he did not have the opportunity to talk to me earlier. My first impression is that as soon as he feels lonely and needy he wants to talk to somebody. Then he tells me he has checked out of the in-patient clinic and has found accommodation in a hostel of the Salvation Army. The previous weekend he felt very lonely there, although the director took care of him very much. He tried to hang himself with a cable but did not succeed. Mr. H. informs me about this completely without emotion. He explains that he was missing the warming atmosphere of the ward.
The following three conversations are underpinned by an event that is still disturbing Mr. K. very much. He tells me that his ex-girlfriend offered to cook for him at her house on his birthday. He went to her house at the time agreed upon, but she did not open the door. He called her from a public phone. She answered the phone and told him she was still in bed. It was clear to him that she was in bed with her current boyfriend. He felt like being kicked onto the street. After his initial fury he felt "like in a film", so humiliated. She apparently showed no empathy at all. He felt so unprotected having disclosed his wishes to her so sincerely that now he could only "completely shut himself down" again. All he is now seeking is calm, he says, and finally the inner film will stop. What he finds particularly bad is that now he has nobody to take care of his dog, because he has become so dependent on his girlfriend. Every time he has to go to her house to fetch the dog, he feels extremely mortified and humiliated. Mr. H. obviously spends almost all of his time thinking about his dog being looked after. His dog symbolizes the part of himself not being currently attended to. As a consequence, he has fallen into a state of inner unrest, and he describes this as an undifferentiated physical condition. He has started drinking more and more beer in the evenings to calm himself, at least a little. At the end of the fifth session, I mention the possibility of a medical treatment, as I could see no way of easing the effects of the conflict with his girlfriend. This he felt as a rejection, and it must have reminded him of an earlier, similar experience. I suspect these "on and off" - changes with his girlfriend are something he initially experienced with his mother. I also think the separation from a woman unconsciously means death for Mr. K. (see the parallel to his father who died after his mother had left him).
History of suicidality
After the separation from his girlfriend Mr. H. swallowed a mixture of tablets together with alcohol while sitting in a taxi. He then fell asleep. However, he had not switched off the radio so that the taxi centre noticed he did not react and tried to track him down. Somehow he got into the clinic.
He could not stand being rejected so massively, having disclosed his innermost feelings to his girlfriend so sincerely. He felt he had no place in this world any more. He has always experienced a longing for death, always being beneath the surface. The experience that nothing good or nice is permanent for him and that in the end he is always left alone is not bearable for him any longer.
Biographic details
Mr. H. grew up in a small town in northern Germany with his parents and his brother, who is five years younger than him. He remembers his youth in this small town mainly as a time when he was part of a music scene with friends, a phase symbolising for him an independent way of life he now misses. The family lived in large premises where his mother's parents also stayed in a house. His father ran a photo shop on the premises. The grandmother dominated the clan, whereas the father spent much time in his shop, using it as a place to retire to. He was always in a state of slight inebriation, apparently feeling constantly under pressure to be successful in his job. As a child Mr. H. used to tinker a lot in his father's shop. The atmosphere in his family was stamped by his "rustic father" and his beautiful mother, who came from a civil servant's household. During his last years at home the relationship between his parents continued to deteriorate. Finally his mother divorced his father, whom she eventually came to despise. After the divorce his father was in a very bad state of mind. When he (the patient) once went home for a visit (he worked for the alternative civilian service in Husum at the rescue service5)), he found his father dead. He had apparently "croaked", as the patient said, from too much alcohol. After his civilian service his mother obtained an apprenticeship as a TV-technician for him, which he finished. Later he worked in this profession at the Federal Post for 7 years until he had problems with his back, which made it impossible for him to work in that job any longer. A friend from the music scene had convinced him 2 1/2 years earlier to move to Hamburg with him into a flat-sharing community. That friend was a heroin addict and is now dead. Other friends of his died of AIDS. He feels he has experienced so many separations and deaths that he has lost all hope that anything good can last.
In Hamburg he worked as a free-lancer for an artist for some time, living on his premises in a mobile home with his dog. When that artist could not pay him any longer, he started working as a taxi-driver. He has known his (ex-) girlfriend for six years. She is a very active woman who sometimes reminds him of his mother. They (he and his mother) understand each other very well. His relationship with his girlfriend, however, is characterised by ups and downs. She often finds he is lacking initiative and sometimes completely spoils the atmosphere by her reproaches and bossy behaviour. On the other hand, he appreciates her domestic abilities. She has a nice flat and he very much enjoys having meals with her. But he does not feel he can really relax there as it is not his flat.
Appendix 2: Protokoll des Fallvergleichs und der Identifizierung prototypischer Fälle in Hamburg [Protocol for the Case Comparison Process and Identification of Prototypical Cases in Hamburg]
Das folgende Protokoll berichtet über den Forschungsdiskussionsprozess im Rahmen der Verstehenden Typenbildung zur Entwicklung von Idealtypen suizidaler Männer. Die Teilnehmer wurden mit chiffrierten Kürzeln benannt. Das Protokoll ermöglicht über den Vergleich mit dem Protokoll der Londoner Gruppe einen Einblick in die Ähnlichkeiten und Unterschiede der beiden Diskussionsprozesse des gleichen Materials in Hamburg und in London.
Zusammenfassung des ersten Diskussionstages 5.7.2001
Wir begannen mit einer kurzen Einführung in die Bedeutung und Funktion von Idealtypen, wie sie hier verstanden werden, d.h. es geht nicht darum, scharf abgegrenzte Einheiten zu definieren, zu denen die einzelnen Patienten ausschließlich zugeordnet werden, sondern mehrere Gruppen von Patienten zu bilden, die ähnliche Aspekte in sich tragen, wobei diese Aspekte von besonderer Bedeutung für die jeweilige Fragestellung sind: Welche Übertragungs- Gegenübertragungssituationen korrespondieren mit der Suizidalität, welche Aspekte der Biografie sind wichtig zum Verständnis von Übertragung und Gegenübertragung, und welche Aspekte der Biografie sind wichtig zum Verständnis der Suizidalität. Wir begannen mit "Übertragung – Gegenübertragung – Suizidalität". Dies höchst wahrscheinlich deshalb, weil hier die Therapeut/innen ein wichtiges Prinzip der hiesigen Arbeit anwenden konnten, nämlich das aktuelle Übertragungsgeschehen in einen Zusammenhang zu bringen mit der Suizidalität, was ja vielfältige Implikationen für die Einschätzung der Akuität der Suizidalität, aber auch der weiteren Therapieplanung hat. Wir waren also in einem genuinen therapeutischen Bereich. Wir begannen ohne weiteren Hintergrund mit dem im Alphabet ersten Patienten, Herrn R, und stellten an ihm eine spezifische Aggressionsproblematik fest: Ein Mann mit Immunschwäche (HF), ein Kämpfer voller Misstrauen und rasch paranoid in der Übertragung, was auf eine frühe Störung hinweist. In seinem Erleben kommt "die Schwäche von außen", man hat ihm etwas angetan, darüber ist er rasend wütend, weil er andere nicht umbringen kann, muss er sich selbst umbringen. Die Aggression ist nur schwer zu kontrollieren, wobei er nicht nur Mörderisches an sich hat, sondern auch Kontakt aufnimmt.
Aus diesen Überlegungen heraus entwickelte sich zunächst eine Gruppe von Patienten mit einem aggressiven Übertragungsangebot, die dann aber noch einmal in zwei Untergruppen geteilt wurde. Die eine Gruppe (D, G, M, R und etwas auch F) ist gekennzeichnet durch massiven Kontakt, mehr oder weniger gut kontrollierte Aggressivität, die im Gegenüber Sorge und Angst erzeugt. Es handelt sich um narzisstische Männer mit einer oral-aggressiven Struktur, die zugleich aber auch "gestandene" Männer sind, bei denen der Suizid nach dem Motto "ein Mann – ein Wort" phantasiert wird. Die andere Gruppe, zu der K, B und etwas auch F gehören, lässt sich charakterisieren als adoleszent gebliebene Männer. Diese stellen eine stärkere Verbindung zum Therapeuten/zur Therapeutin her, wodurch auch in der initialen Situation weniger Sorge um den Suizid besteht. Im Hintergrund ist wohl eine unvollständige Trennung von der Mutter zu vermuten. Die Impulskontrolle ist bei beiden Gruppen gestört, bei der letzteren aber werden die aggressiven Affekte gehalten, solange die Beziehung besteht. Es liegt eher eine oral abhängige Struktur vor.
Innerhalb der "gestandene Männer"-Gruppe zeigte sich, dass Herr R und Herr G zwar optisch ähnlich sind und auch ein ähnliches Misstrauen haben und unkontrollierte Wut. Bei G erfolgte der Verlust mit 7 Jahren. Er muss eine frühkindliche Illusion aufrechterhalten, wohingegen Herr R mit seiner Immunschwäche eine viel frühere Beschädigung erlitten hat und näher am psychotischen Erleben ist. R und K, beide sehr unter Druck, machten hier "viel Wind". R und M sind beide durchtrainiert, "SS-Offizierstypen", der Körper ist sehr wichtig, wobei M etwas weniger aggressiv ist als R und daher weniger "eine Bombe, die nur provisorisch gesichert ist" (ein Teilnehmer).
Eine zweite, sich evtl. überschneidende Gruppe bilden Männer, die "verloren" erscheinen, beziehungsabgewandt sind, den Therapeuten aber berühren, jedoch nicht wirklich erreichen. Hierzu gehört Herr H, Herr Q und etwas auch Herr T, der aber auch etwas von der dritten Gruppe hat, die als adoleszent-abhängig und nicht aggressiv in der Gegenübertragung erscheinen. Diese (N, A, P auch etwas) sind "Riesenbabies", die in Bezug auf die Suizidalität und auch in der Übertragung verdeutlichen: "sie kann doch nicht einfach weggehen und mich alleinlassen". So ist der Suizidversuch stark im Zusammenhang damit, Hilfe zu mobilisieren. Das Leben (Herr P) findet in Abhängigkeit statt. Insgesamt aber eine Reinszenierung früher, infantiler Pathologien. Ausführlich wird diskutiert, dass Herr P ja als älterer Mann nicht mehr adoleszent ist, sondern ganz offensichtlich fixiert ist in einer kindlichen Bindung an die Objekte, die ihn das ganze Leben über versorgt haben, und es wird dann in der Diskussion wieder die Frage deutlich, ob ein früher Defekt überhaupt sichtbar ist, irgendein frühes Verlusttrauma, oder ob er eben nie losgekommen ist. Für ersteres spricht, dass er als kleiner Junge einmal, als die Eltern weggingen, "die ganze Straße zusammen geschrien hat". Dann gibt es noch eine vierte, wieder mehr etwas aggressive Gruppe, nämlich passiv aggressive Männer, wobei diese passive Aggressivität in der Übertragung auch in enger Verbindung zur Suizidalität steht. Unterwerfung als Übertragungsangebot ist dabei vorherrschend und dann das Eingehen sado-masochistischer Beziehungsmuster, die gerade auch in den gescheiterten Liebesbeziehungen eine große Rolle spielten. Vorherrschend ist eher eine anale Struktur. Nicht zugeordnet wurden hier L, S, O, U und I. Bei Herrn I wurde gerade das narzisstische Beziehungsangebot sehr betont, das allerdings nicht in der Übertragungsbeziehung zum Tragen kam. Bei Herrn U die reale Bedrohung durch Verurteilung und erneutes Gefängnis, die ihn suizidal werden ließ und eine Übertragung, in der die Verführung und das rigorose Nichtannehmen dieser Beziehungsaufnahme durch den Therapeuten eine Rolle spielte.
In der Mittagspause diskutierten wir beim Essen die Frage, was eigentlich der Sinn dieser Idealtypenbildung ist (LQ6)). LQ fragte, warum nicht einfach eine gute psychoanalytische Diagnostik mit einer Aussage über Struktur, Abwehrkonflikte und Übertragungsangebot ausreichen würde, um die Patienten zu verstehen. Demgegenüber stand die Argumentation, dass es sich um eine "Findeforschung" handelt, d.h. dass zwar mit einer vorgegebenen theoretischen Orientierung gearbeitet wird, es aber trotzdem möglich ist, neue Aspekte der Suizidalität und der Beziehungsaufnahme mit suizidalen Männern zu beschreiben. Zudem lassen sich hier durchaus auch unterschiedlich "gefährliche Formen" von Suizidalität in der therapeutischen Beziehungsaufnahme darstellen und Aussagen machen, die weniger in Richtung auf die Psychoanalyse als in Richtung auf das Verständnis von suizidalen Männern im medizinischen Bereich gerichtet sind. Denn es wird deutlich, dass hier gerade nicht "he died for glory"7) eine hervorragende Rolle spielt, sondern schwere Pathologien und schwere Beziehungsstörungen. Letztlich aber ist die Kritik nicht völlig von der Hand zu weisen, und wahrscheinlich muss in der Diskussion darauf hingewiesen werden, dass auf diese Weise doch unterschiedliche Behandlungsstrategien aus solchen verschiedenen Typen folgen.
Am Nachmittag wurde es dann sehr anstrengend. Wir beschäftigten uns mit der "Achse" "Biografie – Übertragung/Gegenübertragung" und gerieten in eine Diskussion, inwiefern überhaupt zur Identifizierung und Beschreibung von Übertragungsgeschehen die Biografie notwendig ist. Ein Argument (HF, LQ) war, dass wir die Details der Biografien ja gar nicht genau kennen, insbesondere gar nicht genau wissen, welche Bedeutung diese für die aktuelle Übertragung hat. Es ist also offen, ob die Aspekte der Biografie notwendig oder nur hinreichend sind. Wieder entbrennt diese Diskussion anhand des Falles R und der Frage, ob nicht nur die hochambivalente Bindung an die Mutter sich in der Übertragung widerspiegelte, sondern auch die Tatsache, dass der Vater starb, als er 10 Jahre alt war. OF war der Ansicht, dass man gewisse Übertragungs-Gegenübertragungsphänomene nur kennzeichnen kann, wenn man es auch biografisch belegen kann, wohingegen HF Gegenübertragungsphänomene dann erlebt, wenn er diese Gefühle als fremd von der eigenen Person erkennt und bemerkt, dass etwas vom Patienten ausgeht, was in ihm etwas auslöst. Die Deutung müsste dann im Hier und Jetzt erfolgen. Wohingegen OF der Deutung etwas "Ursächliches" beimaß. Für QK entstand die Angst, dass wir uns in eine Grundsatzdebatte verstricken, in der Teile der Gruppe es ablehnen, sich überhaupt Gedanken darüber zu machen, was an der Biografie die Übertragungsbeziehung denn charakterisieren könnte. Er versuchte deutlich zu machen, dass die Patienten ja uns ihre Fakten als "hängengebliebene Deckerinnerungen" präsentieren und sie sich auch über den Kondensierungsprozess hinweg in uns weiter manifestiert haben (sicher vor dem Hintergrund unserer theoretischen Ausrichtungen), dass sie aber als relevante Hinweise nicht von einer unerheblichen Bedeutung sind. Während dieser Diskussion waren dann schon einige "idealtypische Fantasien" gefallen.
So wurde benannt, dass eine hochambivalente Mutterbindung häufig vorherrscht und ein Dritter fehlt, sodass man in einem ungetrennten dyadischen Zustand verbleibt. Zu dieser Gruppe konnten dann eine ganze Menge Patienten zugeordnet werden: R, K, A, N, I, G und C.
Dann konstellierte sich eine andere Gruppe, wo die Eltern wie ein verschweißter Block erschienen und das Kind außen vor blieb. Gelegentlich war auch dann eine paranoide Übertragung beobachtbar. Hierzu fanden sich dann F, O, Q und etwas auch H.
Eine dritte Gruppe war dann eine "ganz normale Familie", nur das Kind ist psychisch vernachlässigt. Hierzu fanden sich dann L, D, U und S. Andere Fantasien, die dann nicht weiter ausdiskutiert wurden, waren eine ambivalente Vaterbindung oder der nicht zur Verfügung stehende Vater, Adoption (E), Zwilling (B, D). Nicht zuzuordnen waren M und T.
Die Atmosphäre war am Nachmittag sehr angestrengt, es war warm und letztlich gingen aber alle mit dem Gefühl, doch einiges geleistet zu haben. Als Sonderfall entpuppte sich immer wieder H. LQ fühlte sich häufig nicht verstanden, erwirkte auch noch eine Veränderung im Fallbuch, da sie keine Schuldgefühle H gegenüber hatte, als sie in der zweiten Stunde erfuhr, dass der Patient einen Suizidversuch zwischendurch gemacht hatte, vielmehr stand im Vordergrund das Nichterreichen, das nicht im anderen bedeutungsvoll werden. Nichtvorhanden in der Gruppe der untersuchten Männer sind die "Manager", die Hochleistungsmänner, die sehr bedrohliche Suizidalität haben können, aber offenbar nur in bestimmten Settings auftauchen, wie z.B. als Privatpatienten von OF. Bezüglich der Übertragung-Gegenübertragung merkte OF an, dass die therapeutische Situation in den ersten 5 Stunden nicht unbedingt mit der Übertragung-Gegenübertragung konkurrent ist und noch einmal genauer gefasst werden sollte, was denn hier gemeint ist.
Zweiter Diskussionstag, 6.7.2001
Die Gruppe beschäftigte sich zunächst noch allgemein mit der Übertragung-Gegenübertragung. LQ stellte fest, dass die sich möglicherweise entwickelnden Typen sich nicht auf der gleichen metatheoretischen Ebene befänden. Sie würde gerne da deutlicher trennen, ob man sich auf einer analytisch reflexiven oder deskriptiven Ebene befindet. Deutlich wird, dass die Biografie wesentlich mehr von deskriptiven Elementen beinhaltet (obwohl sie ja durch einen intensiven Filterungsprozess auch schon einem "Verstehen" ausgesetzt wurde), als die Übertragungs-Gegenübertragungssituation, die viel schneller einem deutenden Verstehen ausgesetzt ist. Über die Klärung, dass wir hier zwei Aspekte zusammenzubringen haben, etwas mehr Deskriptives mit einem verstandenen und gedeuteten Phänomen in der Behandlung, stellen wir fest, dass bestimmte deskriptive Einheiten eben nicht die gleiche Übertragungsreaktion bedingen müssen. So stellt sich heraus, dass die Tatsache des Vorhandenseins einer hochambivalenten Mutterbeziehung und des Fehlens eines Dritten, so dass ungetrennte Zustände aufgesucht (oder gefürchtet) werden müssen, zwei verschiedene Übertragungsmodi zur Folge haben können, nämlich einen objektabgewandten Modus, wenn der Patient sich abgelehnt fühlt oder ablehnend reagiert und einen Modus der Verschmolzenheit, bei dem nichts Drittes toleriert werden kann. Dies bringt dann diese recht große Gruppe, die dahinter steht (G, C, K, A, I, R, N) zumindest dann der Gruppe näher, die sich von ihren Eltern ausgeschlossen fühlten, wenn der objektabgewandte Übertragungsmodus vorliegt. Dann können die anderen 4 Gruppen relativ rasch gebildet werden. Allerdings fällt LQ in der Diskussion eine Neigung auf, dass wir uns ja normativ verhalten, so diskutieren, dass bestimmte Aspekte nicht geschafft wurden in der Biografie. Auch fällt auf, dass kein homosexuelles Übertragungsangebot vorliegt, was darauf zurückzuführen ist, dass keine Patienten mit reinen homosexuellen Strukturen vorlagen.
Die Diskussion um die Achse Biografie – Suizidalität gestaltet sich dann zunächst auch wieder sehr schwierig. Wieder fällt uns auf, dass wir die Suizidalität ja deuten können, sie jedoch nicht in ihrer Phänomenologie einer bestimmten biografischen Konstellation zuzuordnen ist. Auch fällt auf, dass es eine große Gruppe Männer gibt, die zur Biografie wenig sagen, also eher ein Mangel an ausdifferenzierter Objektrepräsentanz vorliegt. Zunächst wird eine Realtraumatisierung beschrieben, die man unter "Adoption" – frühe Ablehnungssituation und -Fantasien beschreiben kann. Hierunter fallen die beiden (abortiv) adoptierten Patienten K und E auf, die früh so abgelehnt wurden, dass ein (Über-) Leben mit der Mutter nicht möglich erschien, und die sehr räuberische Beziehungen eingehen. Suizidal werden diese Menschen bei Entwertung, beim Bewusstwerden ihrer räuberischen Art, Beziehungen zu leben. Dann aber ist die Diskussion sehr stockend. Wir diskutieren nacheinander mehrere Fälle durch und kommen zunächst nicht zu allgemein gültigen zuzuordnenden Einheiten, bis die Vorstellung aufkommt, dass der Einbruch von Realität bei bestimmten Männern mit einer narzisstischen Problematik die Suizidalität auslöste und diesem Einbruch der Realität nichts mehr entgegengesetzt werden kann. Biografisch herrscht dann ein Gefühl, nicht gewollt zu sein, ein Mangel an Präsenz, Erkennen- und Gehaltenwerden durch die Eltern und eine Reaktion, auf diese Art Erfahrung der Ablehnung durch die Eltern mit einem Gefühl zu reagieren, selbst nichts wert zu sein. Hierzu lassen sich dann am Ende relativ rasch die Herren G, C, I, N, M, A und T assoziieren. Am Ende bleiben noch einige mögliche Gruppen offen. Da ist zum einen "Krankheit – Behinderung und ihre Verleugnung" (R und S) und zum anderen ein Verlusterleben – "ich kann nicht allein sein", ohne dass narzisstische Entwertungen der Objekte erfolgten, einfach ein Wegbrechen für überlebenswichtig gehaltener Objekte und das Gefühl, dies nicht überleben zu können.
Protokoll zur Prototypenbestimmung am 8.7.2001
Zunächst diskutierten wir nochmals die Achse Biografie – Suizidalität. Den größten Bereich machten die "Narzissten" aus, bei denen die Suizidalität auftritt, wenn die Realität hereinbricht und ihr nichts mehr entgegengesetzt werden kann. Größenfantasien können nicht mehr aufrechterhalten werden, Aggression tritt als Symptom auf. Der Patient gerät in ein Erleben von zeitloser Gültigkeit, "so war es immer". Biografisch lag ein Erleben, so nicht gewollt zu sein, vor, aber auch zumindest teilweise aggressive Auseinandersetzungen der Eltern, frühe Gewalterfahrungen und eine frühe ohnmächtige Wut. Wieder wird deutlich, dass hier einerseits biografische Angaben interpretiert werden, insbesondere fällt auf, dass manche Männer dieser Gruppe über ihre Biografie sowieso sehr wenig berichten können, wahrscheinlich, weil sie die frühen Objekte so wenig differenzieren konnten und wenig davon in sich tragen können. Den "Adoptionstypus" trennen wir noch einmal auf und nennen ihn einerseits "Realtraumata" mit der Beschreibung, dass der Mensch sich so früh abgelehnt fühlte, dass ein Überleben mit der Mutter nicht möglich erscheint. Auch hier wird wieder deutlich, dass das "Trauma" interpretiert werden muss, dass also nicht ein reales Trauma unbedingt erzählt worden sein muss. K, der auch beinahe adoptiert worden wäre, gerät damit stärker in der Gruppe der Narzissten hinein. Wieder geht es auch um die Frage, was denn in der Biografie wirklich typisch sein muss, um Suizidalität zu erklären, und wir stellen fest, es ist eben nicht nur die "klassische" Situation. Ein Verlust allein reicht nicht, es müssen noch andere Aspekte dazu kommen. AF betont, dass die Suizidalität durch sehr vielfältige Stränge zu erklären ist, wozu ich dann sage, dass dies im Zielscheibenrating8) ja auch herauskommen kann. OF hebt die Aggression hervor, die als Abwehr des Nicht-Gesehen-Werdens auftritt, weil der Patient wütend über das Versagen der Abwehr wird. AF hebt dann nochmals wieder deutlich hervor, dass auch diese Methodik eben nicht Realitäten beschreibt, sondern das Diskursive in den Vordergrund rückt, die Interpretation. Im Text steht manchmal etwas anderes, als im Diskurs miteinander bearbeitet wird, der sehr stark geprägt ist durch das, was der Therapeut deutlich macht, so dass, obwohl es hier darum geht, dass biografische Angaben im Bezug auf die Suizidalität gesucht werden, in den Diskurs auch die Interpretation anderer Ebenen, insbesondere Übertragung/Gegenübertragung mit hineinfließen. QK führt dazu noch aus, dass der Diskurs hier im wesentlichen auf eine Einigung zielt und zwar den Wunsch, etwas Allgemeineres zu finden. AF sucht dann noch einen anderen Ansatz, wie: wer tötet wen oder was? Es wird deutlich, dass dieser Ansatz eben nicht der einzige ist, mit dem diese Achse untersucht wird, aber durchaus mit in die Diskussion einfließt. HF hebt hervor, dass die Biografie nicht etwas über die Struktur aussagt, sondern dass die Struktur-Diagnose im wesentlichen aus der Analyse von Übertragung/Gegenübertragung erfolgt. Die inneren Objekte findet man eben nur in der Übertragung, woraufhin er die Begrenztheit der Verwendung der Biografie betont. AF führt an, dass die meisten, die Suizid machen, dies meistens nicht in einem Resümee tun, sondern im Rahmen einer aktuellen Sicht auf sich, die sich auch ändern kann, wenn der Suizid (versuch) überlebt wird. Diese aktuelle Sicht sei es, die erfasst wird, wenn man den Zusammenhang zwischen Biografie und Suizidalität darstellen will. FE zeigt auf, dass es Aspekte gibt, die alle Typen einigen, insbesondere den Aspekt, dass die Eltern einen nicht wahrnehmen und dann eine Identifikation mit dem Gefühl unwichtig und wertlos zu sein auftritt. OF schlägt dringlich vor, die Diskussionsgruppe genau zu beschreiben und genauer auch darzustellen, dass der Therapeut sehr häufig in der Gruppe zum "Anwalt" des Patienten wird. Die Gruppe setzt sich also aus Therapeuten, Diskutanten, des jetzt mitdiskutierenden Therapeuten, aber auch zwei Teilnehmern zusammen, die keine Therapeuten waren, wobei einer (OF) nicht am gesamten Diskussionsprozess des Marathons beteiligt ist. Wir stellen fest, dass die Typologie nicht alles erklärt, sondern besonders typische Aspekte. OF, der nochmals deutlich macht, wie die aktuelle Sicht auf die Biografie zu verstehen ist, bringt das Bild eines Schwimmenden, in Not geratenen, der von einem Boot aufgenommen wird und zum Hergang eines Schiffsuntergangs befragt wird. Wir hören seine Geschichte, sie wirkt auf uns, ob sie wirklich so war, ist das Zweite. Dadurch, dass die Menschen hier in aktuellen Krisensituationen ankamen, ist auch ihre Darstellung der Biografie und die Frage, wie sie auf uns wirkt, spezifisch geprägt. OF schlägt vor, dass die Gruppe (der Diskutierenden) auch dahin gehend identifiziert wird, dass eine klare, psychoanalytisch-psychotherapeutische Identität vorliegt, trotzdem aber sehr unterschiedliche Haltungen und ein unterschiedliches Verständnis der Suizidalität, dass alle gemeinsame Supervisionen hinter sich haben, gemeinsam die Fälle supervidiert haben, und dass alle eine 7-10 Jahre währende Erfahrung mit Suizidalen haben.
Protokoll über die Prototypenidentifizierung vom 7.07.2001
Wir beginnen mit der Identifizierung der Prototypen auf der Achse Biografie – Suizidalität, die wir zuvor nochmals diskutiert hatten. Herr M wird gewählt, weil er geleckt, top gekleidet erschien und sobald es ihm besser ging, wieder sehr kalt wurde und kaum noch etwas wollte. Er habe kein Gefühl für Nähe und Beziehungen, aber wenn er etwas verloren hat, ist er ganz kindlich und verzweifelt. Beziehungen hat er eigentlich als Versorgungsinstanzen erlebt, die Geborgenheit vermitteln sollen, als Tankstellen. Die Bedeutung von gegenseitigen Abhängigkeiten kann er überhaupt nicht anerkennen. Die Konfrontation mit der Realität bringt ihn in eine fatale Lage. Die Freundin ist nicht so dumm, wie er dachte. N hingegen ist ein gescheiterter Sozialpädagoge, auch bei ihm bricht die Realität herein, weil die Freundin von ihm Väterlichkeit fordert und er merkt, er kann überhaupt nicht alleine sein. Offenbar war seine Verfassung schon regressiv labilisiert durch die Geburt des Kindes. OF macht deutlich, dass er 1. versucht, eine brutale Realität zurückzudrängen und 2. eine untüchtige Abwehr hat und meint, im Text sei mehr Aggressives. B erkennt dahingehend vielmehr seine Beziehungsproblematik und dass in ihm etwas Zerstörerisches ist. Aus Angst, dass "sie" sich trennt, muss er der Trennung zuvorkommen. Im Grunde geht es darum, dass der drohende Verlust der Mutter ständig in den Beziehungen reaktualisiert wird Wenn er aber in Beziehungen ist, dann gerät er in einen unterwürfigen, infantilen Sog. O hingegen lebt einen massiven Rückzug, der die Ausgestaltung des Lebens sehr beeinflusst. Auch da ist das Nichtgesehenwerden und Sich-selbst-überlassen-Sein in der Kindheit wohl im Vordergrund. Trotzdem wählen wir F als typischen Vertreter, weil diese Momente noch expliziter in Biografie und Suizidalitäts-Anamnese genannt werden. G ist doch wieder deutlicher "narzisstisch" in der großen Gruppe. Lokalisiert. Er kann nicht allein sein, aber wenn er die Einsamkeit doch fühlt, so muss er trinken oder sich betäuben. Der Vater wird aus der Ferne hoch idealisiert, aber in der Nähe gelingt keine Beziehung. Für die Mutter ist er emotional nicht von Bedeutung. Auch bei der Freundin ist eher eine ferne Beziehung vorliegend. Er "hat einfach jemanden", aber er hat sie nicht wirklich. Der Vater wollte zurück in die Familie, in der es, wie auch für Herrn G, die Fantasie von Wärme und Geborgenheit gibt, aber in der Realität wird dies gar nicht überprüft. Die Freundin ist sehr fern, die Bedürftigkeit muss abgewehrt werden, indem er in Distanz zu den Objekten geht. Dabei weiß er gar nicht, wie viel ihm Beziehungen eigentlich bedeuten und kennt seine Brüche nicht. Das Gefühl, zu versagen und isoliert zu sein, steht im Zusammenhang damit, dass er für die Mutter mit seinen Wünschen und Bedürfnissen überhaupt nicht von Bedeutung war. Sie brauchte ihn für sich, da rettet ihn nur gelegentlich die Fantasie des idealisierten ödipalen Siegers. Wenn er aber allein ist, ist er nichts, wird haltlos leer, und der Suizid dient dazu, diese schrecklichen Gefühle zu beenden und gleichzeitig auch etwas Neues zu schaffen. P ist da ganz anders, ein antizipierter Verlust (sie wird sterben) lässt ihn fühlen, dass sie das einfach nicht machen darf. Er hat eine ungeheure Angst vor dem Alleinsein, weil er nicht ausreichende Objekte internalisiert hat. Dafür gibt es nur wenig biografisches Material, nur die Schilderung des Schreiens, als die Eltern einmal abends ausgegangen sind und er sie nicht mehr fand. Er ist ängstlich und sehr verhaftet in beschützenden und behütenden Strukturen. Das Alleinsein hat er ein Leben lang vermieden, und trotzdem ist Getrenntheit tödlich.
Andere Abstraktionen:
B ist ein Zwilling mit einer sehr ambivalenten Vaterbindung, hat etwas sehr "borderline" Adoleszentes.
H ist nicht verwahrlost, obwohl man es immer wieder denken könnte (LQ). Er organisiert aber sein Leben adoleszent, er kommt immer irgendwo dann doch unter.
I wird doch als schwerer Narzisst erlebt (trotz seiner Jugendlichkeit).
L ist kindlich und bedürftig, man darf ihn eben doch nicht alleinlassen.
N ist ein Riesenbaby. Biografisch findet sich eine "normale Familie", aber auch ein Einbruch der Realität, denn die Freundin fordert ihn als Vater. Die Bedeutung der Atmosphäre ist groß, wie es eben oft bei Adoleszenten der Fall ist.
Q kommt im Entzug, hat einen Hexenschuss und fällt a-verbal IG in die Arme.
R (wird viel diskutiert), er ist ein Mann mit Immunschwäche, ein Kämpfer, voller Misstrauen und paranoid in der Übertragung, was auf die frühe Störung hinweist. Die Schwäche kommt für ihn immer von außen, man hat ihm etwas angetan. Das mobilisiert große Wut, und da er andere nicht umbringen kann, denkt er an Suizid. Von Bedeutung ist psychodynamisch, dass der Vater im Alter von 10 Jahren verschwand, auch eine hochambivalente Mutterbindung und die Immunschwäche. Die Mutter lehnte ihn ab, er glaubt, die Therapeutin lehnt ihn ab, wenn sie sagt, er wünsche ihn auf seiner Seite. Seine Aggressionen kann er nur schwer kontrollieren. Trotzdem hat er nicht nur Mörderisches in sich, sondern nimmt durchaus Kontakt auf. In der Übertragung gibt es etwas Tyrannisches, ein Drängen auf Ungetrenntheit.
S: In der Gegenübertragung wird die Behinderung nicht angenommen, sondern nur das Gefühl, er nimmt dem Therapeuten seinen Platz weg. Er selbst nimmt aber auch aggressiv seine Behinderung nicht wahr.
U: In der Übertragung konstellierte sich die Verführung und weniger, dass er unter sich leidet. Eher pervers, gewissenlos, sein Über-Ich ist nicht ausreichend ausgebildet. Die Suizidalität steht im Zusammenhang mit strafrechtlicher Verfolgung, dem Erleben als Kinderschänder im Knast und dem Wunsch, "seine Ehre" zu erhalten. Die Suizidalität kam dabei nicht recht in die Übertragung. Er will den Therapeuten verführen, der sich dagegen mit allen Mitteln wehrt. Die suizidale Dynamik entfaltet sich doch in der Übertragung, meint OF, dem steht deutliche Ablehnung bei QK und LQ entgegen, sodass wieder bei der Diskussion dieses Falles Uneinigkeit und Dissens in der Gruppe auftauchen.
Bei der Diskussion um die Prototypengewinnung zeigt sich, dass das Engagement der Therapeut/innen (unterschiedlich) groß ist. Bei einem Typus, dem derzeit nur zwei Patienten zugeordnet werden konnten, besteht eine Schwierigkeit, welcher denn nur der Prototyp sein soll, die weniger stark ist, wenn es sich um eine größere Gruppe handelt. AF meint, je näher man dem Zielscheibenrating kommt, tritt der Patient in den Hintergrund und das Typische in den Vordergrund. LQ meint, dass die Abstraktionsniveaus nicht ausreichen und immer wieder unterschiedliche Ebenen der Abstraktion gewonnen wurden. Sie fragt dann nach dem Erkenntnisgewinn dieser Studie9), ob es letztlich nicht ausreichen würde, einfach ein gutes Fallbuch zu schreiben? Man käme nie an das Verständnis des Einzelfalles heran und immer wieder bliebe offen, was und in welchem Zusammenhang gewichtet wird. Demgegenüber hält QK, dass es sich hier bei dieser Methode um den Versuch einer Verallgemeinerung handelt. Es ist ein Schritt hin dazu, aber keine echte Verallgemeinerung, und natürlich muss man auch sagen, dass die Einzelfalldarstellungen in der Psychoanalyse sehr häufig durchaus Allgemeingültigkeit beanspruchen und hier doch mit einem viel größerem Aufwand versucht wird, den Weg zur Verallgemeinerung nachvollziehbar zu beschreiben.
Kurzbericht zur Fallkontrastierung10)
Zunächst werden 3 Stunden lang nach kurzer Einführung von allen Therapeuten auf den Overheadfolien die Einschätzungen von Nähe und Entfernung zu den 16 Prototypen festgelegt. Dabei gehen die einzelnen Teilnehmer sehr unterschiedlich vor. OF ist nach 1 1/2 Stunden fertig. HF fängt intensiver lesend an und wird dann schneller, QK gibt sich die genauen 3 Stunden, teilt sich die Zeit ein und benutzt ungefähr gleich viel Zeit pro Fall, wobei er das Idealtypische in Verbindung mit der Ausprägung des Prototypen betrachtet. OF arbeitet ganz sorgfältig 3 Fälle durch, wird dann langsam schneller, hat aber wohl doch Schwierigkeiten, da er zum einen nicht bei der gesamten Diskussion der letzten Tage dabei war, d.h. die idealtypische Steigerung bezogen auf den Prototyp nicht genau versteht, auch die Fälle nicht so gut kennt, andererseits sehr genau sein möchte in seinem Rating. Auch FE ist viel langsamer, weil ihm viele Fälle nicht aus therapeutischer Arbeit, sondern nur aus den Fallbüchern und den Diskussionen bekannt sind.
Um die Mittagszeit kommt dann die Diskussion auf, ob OF und FE, die keine Therapeuten sind, nicht aus dem Zielscheibenrating herausgehalten werden müssten, wie es angehen könnte, dass der Therapeut mit seinem Votum mit den Voten der anderen Teilnehmer/innen gleichgestellt ist. RL entscheidet dafür, dass alle in der Gruppe bleiben, weil der Prozess der Fallkontrastierung auch wieder ein Gruppenprozess ist, wobei natürlich in der Gruppe der eine oder andere sich mehr oder weniger beteiligt und sein Votum mehr oder weniger Gewicht hat und sicherlich das Votum des Therapeuten ein besonders zu betrachtendes Gewicht hat.
Nach dem Mittag erfolgt dann das Zielscheibenrating, wobei rasch deutlich wird, dass die verbleibende Zeit nicht ausreicht, um alle Fälle nochmals zu diskutieren und festzulegen, welche Ähnlichkeit und Differenz es denn jeweils gibt. Trotzdem ist erstaunlich, dass gerade unter denen, die bei der Gesamtdiskussion im Marathon dabei waren, und dabei besonders die Therapeutengruppe eine hohe "Interraterreabilität" vorliegt. Dabei nehmen immer wieder auch die Therapeut/innen eine Sonderstellung ein. Es scheint so zu sein, dass bei einigen Patienten der Therapeut diesen schützen will, das Bedürftigere eher betont, die aggressiv narzisstischen Seiten nicht so recht sehen mag und sicherlich auch noch Elemente der Gesamtbehandlung mit in die Beurteilung einfließen lässt. Bei einigen Prototypen (z.B. R) wird deutlich, dass Unterschiede gemacht wurden dahin gehend, ob eher die Abwehr oder die narzisstische Kälte oder das Abgewehrte, nämlich die Verlorenheit und Verzweiflung, in das Rating einmündeten. Unzufriedenheit besteht mit der Definition der Motti11) "ein Mann, ein Wort", "Realtraumata", "Adoption", "Zwilling", wobei die beiden letzten gelegentlich unterschiedlicher geratet werden, weil nicht die reale Anwesenheit der biografischen Angabe einer Adoption oder eines Zwillingsdaseins, sondern beim Zwilling das Ungetrenntsein in der Übertragung und bei der Adoption die Wiederholung einer biografisch begründeten Ablehnungserfahrung eine Rolle spielen.
Die Gruppe ist müde und kann sich nicht darauf einigen, noch weiter zu machen, sondern vertragt sich auf den 18.7. von 10.00 bis 12.30 Uhr, um die restlichen sieben Fälle dann zu besprechen.
Protokoll des Zielscheibenratings vom 18.07.2001
FE betont zu Beginn, dass wir offensichtlich am letzten Tag unseres Marathons zeitlich in einen erheblichen Druck gerieten und dabei einige Items mehr oder weniger undiskutiert auf gewisse Mittelwerte festgelegt wurden, ohne dass die Gruppe sich wirklich mit den Festlegungen ausreichend auseinandergesetzt hätte und empfiehlt, die jetzt noch verbleibenden sieben Patienten in Ruhe durchzuführen, was letztlich dann auch gelingt. Es wird wieder deutlich, dass gelegentlich Therapeuten dazu neigen, den Patienten bedürftiger zu erleben als die anderen Teilnehmer der Gruppe und häufiger vermeiden, sich auf Prototypen festzulegen, die entwertende Aspekte in der Gegenübertragung oder aggressive Momente betonen, (z.B. O-HF, I-QK). Der 10tägige Zeitraum zum "Prototypenmarathon" scheint mit dafür verantwortlich zu sein, dass ein Prozess des Vergessens und Strukturierens und "Weniger-an-Details-Verhaftens" eingesetzt hat, aber auch ein Prozess, an dem sich manche Teilnehmer leichter von ihren bisherigen Entscheidungen zugunsten des Therapeuten korrigieren lassen. So scheint jetzt das Votum des Therapeuten etwas gewichtiger zu sein als am Ende des Marathons. Insgesamt muss gesagt werden, dass der Marathon über vier Tage die Gruppe überfordert hat und eine bessere Lösung gewesen wäre, wenn nach Festlegung der Prototypen ein Tag Pause gewesen wäre und dann zwei Tage für das Zielscheibenrating angesetzt worden wären. An diesem Tage hätte man sich erholen können und die Erinnerungen an die Diskussionen etwas sacken lassen können, d.h. in Verbindung mit eigenen Vorerfahrungen, theoretischen Annahmen etc. bringen können.
Appendix 3: London Research: Notes from the Process12)
These process notes are the protocol of the discussion process on the case material of 20 suicidal men, taking place at the Tavistock Clinic, London. The participants were blind to the results of the other case discussion group in Hamburg. The protocol will be compared with the research protocol from the Hamburg group to see the differences and similarities in the discussion process.
Day 1
Discussion began about the material and time table for the day. Everyone from the discussion group had read the case notes. The group felt that all the cases merged into one and that the translation from the German original stood out in the material. They asked what the aims of the session were. One member was unclear about the aim of the exercise, another commented on the similarity of the method to Interpretive Phenomenological Analysis.13) One member decided to get started with the material. The group plumped to begin with Case C.
One member, BL, had made notes on the cases and his method was adopted. The method was to have three sections—biography, transference and suicidality. The group began with the transference, then followed with biography and lastly turned to suicidality with all the cases.
Case C
The question arose as to whether the therapist was male. One member thought that the gender of the therapist would likely make a difference in the transference. The group discussed how to start with the case and decided to brainstorm. The group went through what BL had written for the case. Discussion about under which heading some items should go—e.g. perverse excitement as not "strictly transference"; whether "comes with girlfriend" should be under biography; where presentation to the therapist comes; where symptoms should go (e.g. obsessions). They decided that things that are self-destructive go under suicidality, along with factors that appeared to precipitate suicidal acts. It was noted there are numerous variations on the theme of separation.
The question arose as to whether the group should continue discussing until they run out of ideas. Like IPA, the idea is to unpack every aspect of the materials. Like IPA too, it is better to be over-inclusive than to leave elements out. A discussion followed about German culture and how the meetings might be perceived as more formal (i.e. Mr C) than in England.
Excerpt from transference of Case C
The following excerpts will cite direct quotations from the original discussions:
"Infantile about getting the therapist to look at his body; it is linked to the transference. Does not provoke care or love, but anxiety; actually controls objects. Does being off-sick have a self-destructive element? It was actually self-abuse."
"Aggravating stomach ulcer. Finds it hard to communicate; primitive,physical inside-the-body experiences."
"He actually knows what the problem is. He doesn't tell the therapist what he has but describes the symptoms. It is like a baby—cannot put into words what is wrong—lacks symbolism."
"A powerful counter-transference. The therapist cannot quite articulate it, stops thinking and goes into action. It is interesting how the therapy ends with the therapist saying 'no' ('provokes enactment of rejection' goes onto the board)."
"We wouldn't get to these things as individuals ... we get a lot out of it as a group."
"I want spitting-blood to be put down somewhere (spitting blood put down). It links in with 'lacks symbolism.'"
"He wouldn't be spitting blood and calling the therapist, he'd be down at A&E."14)
"A restaging of mother leaving and of being left alone—under biography left alone by mother. Maybe very intolerant of loneliness."
"Or the feeling of being with an object he couldn't relate to and of being left alone. He feels that the object isn't there for him and he's got to do something but does it in a nasty way. Do you have that down?"
A member of the group asked at what risk and how suicidal some of the cases were; there were some that she was very worried about. It was decided that it might be useful to select a theme for the case—"spitting blood"—which was written at the top of the sheet so they can be differentiated.
During discussion of the case, an issue arose: we wouldn't get to this as an individual; we would get a lot more out of it as a group. Picked a theme for the case (e.g. spitting blood). Decide to go on to another case, one of the young ones, it was either A or B, and arbitrarily decided on A.
"Shall we go on?"
"Let's do another one, one of the young ones."
"A or B?"
"Which one?"
"Don't mind. Let's go for A. I call him 'Motorhead'!"
Case A
Named him straight away. The age goes up on the board and the number of sessions; same done for the previous case (C). The group wondered where do things go again; e.g. difficulty leaving home is this better located in biography or transference. BL reads through what she has for this case. "More insight than the other chap".
Transference
"Scooped off the floor back to mummy. A big body builder. Incongruence." "Heavy metal/Motorhead/baby."
"Says of course didn't take it seriously." (not taken seriously)
"Humour in the therapist's account; an adolescent quality."
"He filled the room with music and materials. A compensation for feeling a bit exposed."
"A bit like armour."
"Like an adolescent/child wanting to show off—wanting to show off equipment and girlfriend." (lots of equipment/compensation)
"Picture on T-shirt reminder of something more sadistic when so charming."
"Appointment on birthday." (relative importance of birthday)
"Not sure which communication to listen to, an inauthentic smile for something more destructive."
"Mocking but can get lost in something."
"Sweating, can talk about body."
"It's body communicating (sweat) again."
"No linking with this man."
"Maybe with sweating, does have an effect."
"Is it a link if it's not conscious?"
"It's not very far under the surface." (transparency of defences)
"Unlike the other one, thinks that the therapist likes him (therapist likes him) but then when does get something, that other part of him comes in, Motorhead, and it's all gone. Warning (chilling), can't compete with others for attention."
Biography
"... doesn't use vocational training."
"parents separated when 16."
"parents suicidal. Parents asked for patient to help."
"So murderous."
"Sister psychotic, girlfriend psychotic."
"Mother threatens to kill herself if he leaves."
"Mum is Motorhead ... an external mother that threatens but similarly an internal mother who threatens and kills." (something tyrannical internally)
"Unrealistic liaison with best friend's wife."
"Career progression. Tries to get out but can't, arthritic knee, off sick, unsuitable work."
"Split-off aggression seems adaptive regarding history with parents and must have been dangerous to have a career. Parents very aggressive?."
"How did he adapt to emotional life at home."
"Completely chaotic family."
"No mean feat, he was never good at school. Significance of being able to learn at some point."
"Still looking for something in therapy." (still searching for something)
"Resilience. Expect no bits of help but there, leaves question of why. A good object somewhere."
"Melancholic and smiling. Knows the body aspect as well. Quite insightful in some ways."
"Knows the nature of his defences—i.e. the body and the incongruity between depression and smiling."
"Wish I knew what the 'obviously' is."
The therapist didn't make link with birthday, which is interesting."
"More of a cutter-offer than a colluder."
As the discussion goes on, themes are selected out from the discussion of the case.
|
"Case A"
|
"Motorhead" |
27 years old, 28 sessions Therapist—female |
|
Biography |
Transference |
Suicidality |
|
Dad 53 at birth Significant mental health problems, admissions into psychiatric hospitals "Interruption or stagnation in development "Welded to mother" (HC intervened) Alcohol (parents/him) Bright but does not succeed Does not use vocational training Parents separated 16 Parents suicidal—father asked patient to help Girlfriend and sister Psychotic Mother threatening to kill herself if he leaves Unrealistic liaison with best friend's wife Tries to get out but cannot Arthritic knee, off sick, unsuitable work How did he adopt to emotional life at home Completely chaotic family More of a "cutter-off" than a colluder Significance of being able to learn at some point Resilience Phones for appointment himself |
Smiling/beams—incongruent Unauthentic/untrue Appeal for parental protection (Session 1) Narcissism Attacking/degrading of therapy Ambivalence—does not want to go there—(separation from mother presentation) Incongruous—heavy metal/Motorhead/baby Not taken seriously Humour in therapist's account Adolescent quality Lots of equipment/compensation Showing off? Benign or narcissistic Relative importance of birthday—not commented on by either Can get lost in something/schizoid Body communication (sweat)—is a link, if not conscious? Transparency to defences Therapist likes him Warning (chilling) "can't compete with M.H." Brings girlfriend—evidence of something/aspect of himself? Aggression split off Counter-transference bored/tired but also charmed (either an alliance/defence) Something internal tyrannical Still searching for something Knows the nature of his defences, i.e. body and then incongruity between depression/smile What gets projected into what is around him Does not talk directly about history but in material (society, sweating) |
Birthday Suicidal thoughts and fantasies since youth Nirvana 1 attempt, pill and alcohol (symbolic?) (more serious, dissolves conflict) Not taken seriously, taken "home to mother"—by whom? himself? staff? What does a suicidal act mean (in the family context) Defensive armour Difficulty in separation, being "too dependent" Ends up back with mother, not separated Relief/urgency in first communication |
Table 3: Initial comments and themes from discussion of Case A under the three headings: biography, transference, suicidality
The group next decided to move randomly to Case D.
Case D
How representative of the suicidal population in Hamburg are these?
Suicidality
"Chronic use of sleeping pills and alcohol."
"The therapist does make contact when more assertive and real."
Are we done?
"When she does touch him ... wonder if impacts on how he is feeling?, is it affecting her. A flicker in him of something more realistic. Can she bear him?"
|
Case D |
4 litres of Beer |
39 years, 22 sessions therapist—female; AF; |
|
Biography |
Transference |
Suicidality |
|
One of twin Family split Allied—mother Twin—father Wealthy background "Shy, the loser, good for nothing." Relationships Marriage (Impotent—prostitute) Occupation Optician—functioning well?
|
Large shouting baby Histrionic Ridiculous quality—hard to take seriously Uninhibited Maniac quality Excitement—intimacy sexualised Infantile state/frenzy Merger fantasy Another aspect—functioning optician Parody of erotic transference Fetishising relationships Cannot "do" frustration (oedipal) Block to relationships Threat of abandonment Desperate when separated Fetishises intimacy Role of excitement—enjoyed Impact between he arrives Where is the shyness Plebeian—mocking Therapist does make contact when more assertive/real Can she bear him? |
Acute episode suicidal feeling Alcohol/sleeping pills Precipitated separation from girlfriend Chronic use—sleep/alcohol Previous behaviour? Promiscuous Mother |
Table 4: Initial comments and themes from discussion of Case D under the three headings: biography, transference, suicidality
Someone who fantasises about suicide, rather than someone who has actually done it. The only predictor of your future is your past. Discussion about self-harm; a significant middle ground. Comments that thought it would be a post-mortem. Less inner-city.
Case E
"Made such a difference reading the biographical notes to what had read before—when found out that he was in care, had a different view on relationship than the other one. Impossible to understand patient or patients without the biography."
"Some don't have detailed biographies."
Decided on F & L for the next day and then move on to another three (G/H/K)
Day 2
Start with Case F.
Case F
"Quite a description" (repulsive)
"Some have a lot of images of the body" (body dishevelled)
"Dead"
"Making himself repulsive in one way, a bit of identification as something rather enjoyed about the exclusion" (excluding; victim + rebel)
"No expectations" for "himself"
"Hard to get a sense of the meaning"
"Came across differently, more isolated and quite tied up with his mom & mom had set it up."
"Talked to as more integrated than he was; I thought that he was more fragmented."15)
"Nice description, panic with silence—boredom/contemptuous—that projection of aggression and contempt that keeps him distant from the world."
"Not somewhere where it's knowable to him—something he needs to do—a defence."
"Story of the psychiatrist; fits with L, much more disturbing underneath."
"Not treating a good object badly."
"In a more persecuted state." (Persecuted, isolated)
"A bit paranoid as well." (Paranoid)
"Not right to be here; find it difficult to like him."
"Can engage others to be interested, but doesn't think that he is interesting to others."
"With this one, felt could formulate more, more clinical; could diagnose him."
"Felt more distant—how it's written?"
"Therapist trying to see as more neurotic, the interpretation didn't means things to this man, trying to be put into the wrong category."
|
Case F |
Mr Dishevelled |
30 years, 85 sessions, therapist—male—QK |
|
Biography |
Transference |
Suicidality |
|
No intimate relationships/sex Isolated Mother sets up consultation 2 siblings—rivalry Mother's psychiatrist Cold heartless mothers Welded to mother? Depressed? Father major Mother's assistant Parent's relationship difficult Failure to thrive Aggression in childhood |
Repulsive Body: dishevel Dead, no expectation Excluding Victim + rebel Fragmented Feels persecuted Isolated internally Paranoid Engaging but not recognising Aggression Destructiveness Lack of symbolism Pushing away |
Cut wrists with razor to find out how much it hurts Finding something Following rejection from therapist Deficit Criticism—suicidal thoughts Celebration—jumping Envy? Weight loss |
Table 5: Initial comments and themes from discussion of Case F under the three headings: biography, transference, suicidality
Comments that were made
Does the way the case report is written change anything? E.g. feeling more distant.
Issues of translation.
The number of sessions he stayed for.
Lots of welded (undifferentiated from) to mothers (generalised observations)
Case L
Transference
"There's almost a sense that the children don't exist—and they don't seem to have a presence in his mind."
"The therapist is racing ahead."
"Elicits quite a reaction from the therapist."
"Think something is being re-enacted, I think it's rejection. Passivity/irritated, to elicit quite a cruel reaction."
"Don't know if I agree—agree he's irritating but biography—something of an object that cannot see."
"Not an adolescent patient but a grown man with children."
"Therapist worries about children, not patient."
"Not being able to bear just how disturbed he is."
"Think he's terrifyingly cold—a placidity about him."
"Stirred up in therapists, not just provoked into irritation but something that is intolerable."
"A stupidity or clodidity is such an aggressive defence—not able to see the destructiveness but the core deficit—why does he have to be such a cold clod."
"I wonder if he is a bit stupid."
"An arrested development feel."16)
Biography
"Youngest of five brothers—oldest and 20 years."
"What would German families be like in 1951?"
"Childhood 'very nice.'"
"Getting so easy, because anything difficult is wiped out, and really wiped out. It's flat, one-dimension, get sense of something dangerous lurking—dismissive/avoidant—links with angry parents."
"Post-war Germany. It must have been hard to raise a family. Some are post-war babies. Easier for patient."
"A lot written on post-war but don't seem to come out in the patients."
"Something about children. Is it Catholicism or not able to manage contraception."
"Feel like accessories."
Suicidality
"In response to the rejection. It involves alcohol again."
‘When his being-stupid defence doesn't work again and a cord to hang himself with."
"Maybe a sense of being a benign object."
"Aware that something is amiss."
"I wonder about what he thinks he wants."
"Youngest child, investment in being the baby."
"Get a sense he doesn't know what he wants, doesn't regress to such a passive state—like he wants something to link, but not knowing that he wants someone to link."
"Maybe does want to be picked up, like the youngest children but therapist presently wants him to be a man—maybe took something in—maybe enough."
"Get a lot of babies, but it is a stupid defence."
"Clod will bring it to mind—clod baby."
"Provokes a negative reaction in the therapist."
"Felt with others that not much linking is taking place."
Comments and Observations
Comparisons, similarities and differences made between this case and the other cases (e.g. being welded to the mother). Or, between this case and one other case.
Descriptions so short—the Hamburg group had the therapists there.
A theme is the lack of a capacity for concern and this was proposed as being applicable to all patients.
What would German families be like in 1951? Hamburg suburbs.
Post-war Germany, must have been hard to raise a family—some are post-war babies—easier for patient.
Comment that we have now done two cases. As agreed at the end of the day yesterday, we would stop and think about where we had arrived at.
Should the next stage be to condense them? Repeat the process for each case to condense them? Get best exemplar case—work out prototype case. Should we be forming one prototype? Looking at aspects of the transference—and trying to see how all the cases fit with this at this first stage.
Brought up themes such as victim aggrieved, projection of aggression, repulsion, and then slotted the cases into these, and writing up aspects of the counter-transference (which was added to as time went on). Then gone broader and see which ones are similar to others. People deal with the same problem in different ways. CBT17)—vertical arrow—down to core beliefs.
"It's a sense of rigidity. In the discussion, we've become polarised."
"It arouses a lot of feelings in the therapist that aren't very comfortable."
"If you can get to the deficit, you can understand the destructiveness."
"Is it about a deficit that they're aware of."
"We haven't spoken about separation."
"Therapists invited into the counter-transference about separation—get propelled into something very quickly."
"More an enactment than a counter-transference."
"The therapist must have a different view."
"Must wish to be with the therapist."
The therapist can't quite have a"'third", which links in with the rigidity in the patients."
"Should we summarise the themes—should all the Bio/Trans/suicidality link?
Having difficulties holding onto the child being looked after; keeps on slipping out of one's mind."
All leave for a break.
Case H
"Unlike others, can talk about it but doesn't want to work with it." More comparisons made.
"Similar to other cases—feels humiliated and mortified."
Goes back to the overall themes and then back to the case—continuing the comparison with the other cases.
"Bringing pathology but not aspects of their functioning."
"In the Hamburg team, therapists might champion their case and bring in warmth. Discussion about who we are interested in or warming to. One thing they all have in common is that they came to five session and presented themselves.'
"But they would have been excluded otherwise."
Discussion about the cases, and how they would have been excluded if they hadn't had five sessions. We have given them awful names. Discussion about who we are interested in/warming to.
Plan for next week—choose them and champion them for Monday. Picked which cases we want and don't want to champion for Monday, including the ones that we have already read through.
Tidying up the way we are thinking about the transference and counter-transference section. Colour coding and grouping them. Difficulty grouping—ended up theorising so kept to main themes (c.f. IPA). Trying to give titles to the themes.
Feeling pleased with how it's come together. Interesting when we look at suicidality and biography; slowly starting to encapsulate it, but they do manage the problem differently. Things that we had forgotten started to be remembered and are going back in (e.g. deficit vs. destructiveness).
Everyone was allocated the cases—all were covered.
Day 3
Read through the ones that were selected. Items that struck people (e.g. separation crisis).
"What struck me from the ones I read was a separation crisis. Something about chronic suicide and neglect."
"Quite a lot with drug and alcohol attempts."
"Method I suppose."
"There were some very different methods."
"More overdoses than anything else—some hanging, electrocution, cutting and self-harm."
"Guilt seems to play a part."
"A lot seems be a response to frustration."
"Coercive."
"Spitting blood with girlfriend."
"Mr Dishevelled at the dinner party."
"Also object relatedness."
"There are some that seem just so murderous and killing off an object. With respect to fantasy in relation to a Christian death. Free and secure—a suicide would bring freedom."
"Also, parents who had made an attempt."
"Do we have anything about the idealisation of death?"
"Yes, in Case H."
"Something quite masturbatory about it but less than we would have expected."
"Have you got the cut-off bit category."
"Ability to elicit concern in others. Man passing on street."
"They're not shocked by their suicide attempts."
"You could feel horrified, hanging when he thought he was alright."
"Something about splitting."
"Something about cruel neglect. Wonder if it's a bit defeated as well, though—thinking of defeated and lost hopeful expectation, how many into therapy and think helped, something very tiring."
"Hard to keep their individuality in mind, that's exhausting."
"Still find it hard to keep them in mind. There were merging between them."
"Brought up merging before."
"Don't feel sympathetic with predicaments."
"Something about having to make room for 20."
"Must be like that working just with suicides."
"The therapists not being shocked?"
"We might react rather differently."
"Maybe underestimating how long some of them stay. Might be interesting to see how long a therapy they're offered. I'm confused about what one knows and doesn't know."
"It's also an attack on one's health."
"We wouldn't know the quality of that attack without the transference and questions we're being asked—how they link but didn't feel like we know what it's like in the room—didn't feel like enough of a flavour of what it is like in the room with the patient."
"We would need to know more detail."
"Getting a lot more from current relationships rather than what's happening with the therapist."
"Probably would have been inpatient if they were angry—working out who the patient group was."
"A difference between those that fantasised about it and those that had actually made an attempt."
Comments
General discussion: overview of feelings towards cases; then began to draw on cases that fit these general observations, drawing on cases much more. Exhausting to keep their individuality in mind—merging between them. Comment that we wouldn't know that quality of that suicidal attack without the transference and question we're being asked. The feeling that we don't know what it's like to be in the room. Getting a lot more from the current relationships rather than what's happening with the therapist. Would have been impatient if they were angry.
"Could take the CPA18) approach, categorise in terms of risk." One member went through what the risk factors were—previous attempts, severity, hopelessness, cut-off, isolated etc.
"Couldn't get to certain things in five sessions" (regarding the issue of early abuse that was raised).
"The crunch is when the other person leaves. Will always have to account for the psychopathology of the other—feel like need a couple assessment."
"In some way to become a victim of his own actions and something that he's doing to himself."
"Less able to relate to objects. Complete lack and loss of hope."
"If had object relatedness."
"Not saying 'no' murderousness in that group but much more diffuse and scarier."
"One where a patient is getting better."
"Degrees of sadism."
"Underlie object related but maybe something internal as well."
"How do we do this?"
"We can build up the categories and then still have the information for an ideal type."
Discussion
Discussion about what's green and what's red—going through these colour codings as a group.
"Biographies going to be very hard to do without it being extremely complicated."
"Raised that we could use sub-headings."
"Mother, father, siblings, current relationships"—writes themes on the board, group draws themes from the large descriptions on the wall.
"How can we group them?"
"We can write letters by them—that's what happens in IPA."
"Looking at what's missing—deaths of mothers, say."
"Is it biography or is it actually thinking about it psychoanalytically."
"It depends on how it's presented."
"Why go beyond what patient has told us."
Added categories as went.
Discussion about the cases—two ways of doing it—go through the three points (suicidality, biography and suicidality), or get impressions of which cases fit together and then draw out links.
Bottom-up or more work for ourselves? Work top-down on a conceptual level?
Not very much time (time pressure came in) to try to do it systematically—make a guess at the concentric rings and plot them?
There did seem to be some disagreement about this—a difficulty in moving forwards—this continued throughout the rest of the session.
There's a problem about moving from the general to the specific. Picked out three elements—1. loner/sado-masochistic, 2. enmeshed and 3. unrealistic and picked out the letters below into one of the groups. Some fit into two groups, but one more than another. Discussion that the three groups are like the core complex. Commenting that "it would be interesting to look at it in terms of the three groups in terms of their suicidality; what we have picked up on is a way of relating in the here and now. Look at what themes in each of the cases link to the loner part."
After speaking about the themes of each of the sections, then we debated with difficulty and then we produced some decisions.
Reflected that we will go into attachment patterns.
"Thought it was different ways of dealing with the same underlying dynamic."
"A lack of process to do the counter-transference."
Therapeutic process; "Hard to keep the individual different but also the stereotyping."
"They're adults and should be responsible for how they behave or who/what they are—a difference maybe with working primarily with children."
"A difficulty knowing how to proceed, would have liked to have asked RL more—but he would like us to build it up ourselves."
SB arrived and spoke about how to proceed and to do the next step, i.e. giving a summary of characteristics you would find with each of the cases and communicate over the summer with author RL. You don't reach a final position with this—think in terms of the replication study—although labelled differently, it's what comes out underneath—a hypothesis at the moment, not testing it. Pretty exhausting, energy sapping. Some bits easy in the group, others very difficult. Given the saturation, these three types, with these themes and these are the prototypical cases. Got troubled by the systematic bit—but putting it up is the systematic bit; pick a case now and then plot it and see what it looks like; falsify it, say, if a case is way out, can reconsider the case. Have to distil down the biography—happens when speak about it, the categories will come out, then go, then pick out the prototypical case and give a story about it. The themes were then listed under each of the headings:
Suicidality linked with object relatedness, affect and suicidal method
Object relatedness:
Separation, projection,coercion, cruelty, eliciting concern, sticking with therapy, merging, rejection, murderousness, protest, cut-off, split
Affect:
Frustration, guilt, envy, excitement, idealisation, death, freedom, release, anaesthetising, shock, anger, defeated hope, attack health, external factors, neglect
Method:
Acute crisis—chronic, alcohol/drugs, attempt to parent, self-harm
|
Relationships—aggression |
Lack of psychological thinking |
Managing separation |
|
Aggression Repulsion/contempt Passivity Victim Aggrieved Shame Not bringing functioning self |
Lack reflection Lack symbolic thinking Concrete thinking Ignoring reality Cut-off Couple/third position |
Merger Welding Fetishising Denying Regressed baby Eroticism (?) Idealisation Body building Passivity Perverse |
Table 6: Transference listed in tabulated form to illustrate in three categories; transference and (aggressive) relationships, lack of psychological thinking, managing separations
|
Mother |
Father |
Siblings |
Current |
|
Cold Enmeshed Physical abuse Suicidal/depressed Alcohol Mental illness Death-ill health Inversion in relationship/confused boundaries |
Peripheral Critical Physical abuse Suicidal/depressed (depress of involvement/lack of protection—witness) Alcohol Death—poor health? Identification, e.g. similar career Mocked fathers—made passive Old |
Rivalry Twins Death of siblings Disability of sibling Large family Favouritism |
General Isolated Few friends—male friendships |
|
Functioning |
Early history |
Girl/Boyfriends |
Quality of history |
|
Sometimes protected—high powered Some more primitive level Some have jobs, no changes Some—lots of changes Falling out of education/employment Off sick for long periods of time Neglected accommodation Preoccupation with narrow interest—body building—music |
Adoption Early separation Disability—death Bullied at school |
Homosexuality Promiscuity Impotence Younger GF's S-M relationships Few children Fuzzy separation Affairs Idealisation Older girlfriends Early marriages Few/no relationships |
Missing Dismissive/avoidant19) Preoccupied |
Table 7: Themes and categories across cases, for Biography, Transference and Suicidality
Counter-Transference qualities:
Irritation; Hostility; Enactment; Guilt; Boredom; Maternal; Maternal enactment; Reaction formation?; Self-righteous; Rigid; Judgement; Sledge hammer; Rejection; Mockery; Sado-Masochistic
Biography, qualities and cases:
Case A: enmeshed mother, alcohol, chaotic, development blocked, off-sick (and Case C); suicidal parent; controlling parent;
Case C: cold mother—absent father; success at work; physical abuse
Transference:
Case A: dismissive/degrading, showing off, use of body (and Case C)
Case C: provocative, enactment, perverse
Counter-Transference:
Case A: unauthentic
Case C: hatred,
Suicidality:
Case A: chronic thought, not taken seriously
Case C: self-destructiveness—illness
This can be pulled together through listing themes under four categories, presented below.
|
|
Biography |
Transference |
Counter-transference |
Suicidality |
|
Case F |
No job Sibling rivalry Mother—cold Mother therapy Alcohol
|
Repulsive expectations of therapy Annihilation fear of annihilation of self Projected aggression Can use therapy |
Anger |
Serious attempt Precipitated by rejection, Humiliation, Envy Deliberate self-harm Recurrent suicidal ideation |
|
Case H |
Parental mental health Homeless—rootless Parental discord: Mother despises father Childhood aggression Underachievement Parental mental ill health/death |
Hopelessness Absence of aggression Between patient + therapist Passivity schizoid Illicit concern
|
|
Serious attempt |
Table 8: Themes of biography, transference and counter-transference for "loner" category cases
Day 4
"I think there's another group. I completely agree with the loner group. Loners and schizoids—become quite regressed when rejected and the therapist feels quite worried. Different from schizoid set, not as perverse or cut-off but slightly different reaction to the therapist."
"Don't know why we put M there (i.e. in the sado-masochistic), seems like more of a loner."
"I thought when reading through some more cut-off."
"It's a big group anyway."
"Wondered whether Motorhead was the archetypal enmeshed."
"Thought Mr. Dishevelled was a pretty good loner."
"Wondered why G, thought not so much a loner."
"I still had him as a loner."
"He was the one making a bid for the therapist and analysis."
"Thought S was more a sado-masochistic looking at it again."
"Think aim is to get themes for each of the three groups, get archetypal categories and write a few lines" (i.e. back to aim).
"Think another aspect, not quite a subgroup of narcissism."
"Would have liked to have gone through the counter-transference a lot more—some feel like the therapists just zoned out, trying to re-exert their own boundaries."
"Not sure about intrusive, but rather oblivious—not a directional thing...more his sort of obliviousness to any difference between himself and the therapist."
"Get the feeling that one was much more conscious and another unconscious, where he didn't know that he had relationship or who was pulling the strings."
"Feel quite convinced by SG's baby group."
"I thought your narcissistic group made sense."
"Think might come under the sado-masochistic."
"Think we could incorporate the unrealistic group, it's quite small, only 2-3 cases."
"Like the three-factor model—quite psychoanalytic."
Discussion about whether Case D has an unrealistic theme
"Let's just leave him out."
"There is something that feels different about D. ..."
"Something quite intrusive about him/wants to be in possession of his object."
"The effect of being intruded upon."
"We could go on forever."
"But I do think that there is something."
"Shall we have the withdrawn/regressed and take out the unrealistic group."
Moving of groups
"Shall we try to do it with the other two like we did with the loner" (i.e. the groups)
"I'd like to add something on counter-transference" Going through counter-transference.
"Shall we move on and do as we did with the others?"
"Shall we do the sado-masochistic." Move on to sado-masochistic group.
It seemed that some in the group were finding it hard to let go and move forward.
Doing sado-masochistic group. Trying to put in biography.
"Sorry, getting quite frustrated, afraid going have to repeat what we need to do. Do we have the features of the biography?"
"But that's not specific to the group."
"Ok."
"Feels like we're going to repeat ourselves—we're trying to be more general now."
"The idea is to move from that (the sheets) to there (the thematic sheets)."
Taking the cases we have written up and moving the themes across.
"Hate categorising theme" A difficult thing for the group.
[Including the counter-transference on the sheets]
"Pleased that we have managed to get two that are different, last week we were saying that they were all the same"
"Don't want them to be all different either/social constructivist position."
[Did withdrawn/regressed group]
"You wonder about the girlfriends/why are they with them—a study in itself."
"Feel like if a larger group, a group might be picked up on."
"Something about this group having more investment in therapist; c.f. suicide bombers—i.e., want to get better. Does this link with having a group who have not all attempted?"
[Rethinking about the group. Ended up with 2 large ones and one small one again. Maybe D would be a far distance away from the prototype.] [N.B. D was excluded]
[Going through the loner group.] Looking at the cases to see if any fitted into the withdrawn/regressed group—looked at Case T.
"I still want to lump together the two groups." (i.e. longer and withdrawn/regressed groups)
"Would guess would fit their model of overarching group and then subgroups."
"We've got an hour left. We might have to have some that don't fit well."
"Or three and a subgroup!"
"There is something unrealistic about T."
"A bit more anguished."
"Something that fits in the transference between them as well."
"Move the T with the D into the unrealistic."
"Withdrawn/regressed under loner into a subgroup?"
"Use psychotic in psychoanalytic sense—three groups—withdrawn/sado-masochistic and psychotic."
[Putting letters under themes]
"You might want to have those that are not withdrawn, one group hangs on and one intrudes."
"Solutions to the same underlying problem."
[Fitted them all into groups—left with Case G]
"Thought at times he was trying to be a good/interesting patient."
"I think that quite good."
"Not happy with intrudes."
"Merge."
"Yes."
"More psychotic."
"Not sequential sessions with G—might be why feels different?"
"Think G is acutely interested in what the therapist thinks of him, whereas we don't get that feeling with the withdrawn group."
"What about the psychotic group?"
"Think he's a clingy."
"All ways of managing separation."
[Back to the withdrawn, Cling/Control, Merging—object relating]
[These were discussed and expanded—e.g. control for sado-masochistic]
[G into sado-masochistic. Picked archetypal types for each of the groups]
Joke about being a group experiment.
Picked one word for biography and suicidality for each of these three groups.
[Note: Withdrawn/regressed has been put back with loner]
"Looking at whether cases in the sado-masochistic groups actually have made attempts."
"Few that made suicidal attempts." [Speeding up with aspects falling in]
"Is it object-related in the withdrawn group?"
"Masked attempts/isolated attempts."
Different from the other groups. Looking at the psychotic group for suicidality—psychotic solution. [On checking through them, they seemed to fit/more of an excited feel, everyone seemed pleased with the result]
"Pleased with model."
"Like the difference in quality."
"Shows good inductive thinking that is quite grounded."
Final
|
Type |
Cases |
Object relations |
||
|
|
|
Suicide |
Transference |
Biography |
|
Withdrawn |
E, M, F (regressed), O, P, Q, H |
Isolated, Suicidal ideation, Masked attempts |
Withdrawn |
Loner |
|
Sado-masochistic enmeshed |
L, A, B, C, N, R, U, G
|
Few attempts, object linked
|
Cling/Control |
Controlled, Enmeshed relations |
|
Psychotic-unrealistic |
D, T, K, S |
Psychotic solution |
Merging |
Intense idealised relations |
Table 8: Cases in each category (withdrawn, sado-masochistic/enmeshed and psychotic-unrealistic) for dimensions of biography, transference, suicidality
1) In these terms credibility can be compared with internal validity, confirmability with objectivity and transferability with generalisability. Transferability does not have to become representative, but the practical (or clinical) frame, from which the results are derived should be explained thoroughly (MALTERUD, 2001b). <back>
2) The self-object is defined in self psychology as an (early) object, which is experienced as contiguous with the self, so that the person feels extreme dependency with this object and/or security (BACAL & NEWMAN, 1994). <back>
3) Concreteness means in the psychoanalytical sense: What is real is thought and what is thought is real. There is no difference between inner and outer world and no possibility to interpret the outer world, to find a meaning or an understanding of one's own or the others situation. <back>
4) Nephrology is the diagnosis and treatment of kidney diseases. <back>
5) This is a rescue service on the shores of the North Sea, in northern Germany. <back>
6) Die Initialen der Diskussionsteilnehmer wurden verschlüsselt. <back>
7) In Anlehnung an GERISCH (1998) und CANETTO (1992): "She died for love and he for glory." <back>
8) Siehe Abschnitt 3.4.3. <back>
9) Gemeint ist die Hamburger Studie über suizidale Männer (LINDNER, 2006). <back>
10) Dieser methodische Schritt wurde in der Londoner Gruppe nicht gemacht. <back>
11) Zu jedem Prototypen wurde eine einprägsame Formulierung als Motto gesucht. Dabei wurde manchmal (s.o.) sehr intensiv nach passenden Formulierungen gesucht. <back>
12) Note from the Editors: The protocols provided below are informal and are only partly adjusted to the standards, usually provided in FQS texts. <back>
13) Interpretative Phenomenological Analysis (IPA) is an approach to psychological qualitative research with theoretical origins in phenomenology and hermeneutics. <back>
14) A&E = Accident and Emergency Department <back>
15) "Integrated" is a technical term referring to the inner world. The opposite is fragmented. <back>
16) To have development "arrested" conveys the way that something holds up normal developmental processes. <back>
17) Cognitive Behaviour Therapy <back>
18) Care Plan Approach: a routine way of assessing and managing risks in health service care in the UK. <back>
19) A category in attachment theory, maps on to dismissing. <back>
Anderson, Robin & Dartington, Anan (1998). Facing it out: Clinical perspectives on adolescent disturbance. London: Duckworths/Tavistock Clinic Series.
Bacal, Howard A. & Newman, Kenneth M. (1994). Objektbeziehungstheorien – Brücken zur Selbstpsychologie. Stuttgart: Frommann-Holzboog.
Bion, Winfried R. (1962). Learning from experience. London: Heinemann.
Bion, Winfried R. (1970). Attention and interpretation. London: Maresfield.
Bohnsack, Ralf (2000). Gruppendiskussion. In Uwe Flick, Ernst v. Kardorff & Ines Steinke (Eds.), Qualitative Forschung: Ein Handbuch (pp.369-384). Reinbek, specify country: Rowohlt.
Bouchard, Mark A. (1995). The specificity of hermeneutics in psychoanalysis: Leaps on the path from construction to recollection. International Journal of Psycho-Analysis, 76, 533-546.
Brewin, Chris R.; Andrews, Bernice & Gotlib, Ian H. (1993). Psychopathology and early experience: A reappraisal of retrospective reports. Psychological Bulletin, 193, 82-98.
Britton, Ron (1989). The missing link: Parental sexuality in the Oedipus complex. In John Steiner (Ed.), The Oedipus complex today (pp.83-101). London: Karnac Books.
Britton, Ron (1998). Belief and imagination: Explorations in psychoanalysis. London: Routledge.
Campbell, Donald (2008). The father transference during a presuicide state. In Stephen Briggs, Alessandra Lemma & Will Crouch (Eds.), Relating to self-harm and suicide: psychoanalytic perspectives on theory, practice and prevention (pp.25-37). London: Routledge
Canetto, Sylvia S. (1992). She died for love and he for glory. Omega, 26, 1-7.
Chiles, John A. & Strosahl, Kirk D. (1995). The suicidal patient. Washington: American Psychiatric Press.
Deneke, Friedrich-Wilhelm (1993). Das Selbst und seine Repräsentanzen: Wie kommt der Fall zu seiner Geschichte. In Ulrich Stuhr & Friedrich-Wilhelm Deneke (Eds.), Die Fallgeschichte: Beiträge zu ihrer Bedeutung als Forschungsinstrument (pp.120-139). Heidelberg: Asanger.
Diekstra Rene F.W. & Garnefsky Nadia (1995). On the nature, magnitude, and causality of suicidal behaviors: An international perspective. Suicide and Life-Threatening Behavior, 25, 36-57.
Dreher, Michael & Dreher, Eva (1995). Gruppendiskussionsverfahren. In Uwe Flick, Ernst v. Kardorff, Heiner Keupp, Lutz v. Rosenstiel & Stephan Wolff (Eds.), Handbuch der qualitativen Sozialforschung: Grundlagen, Konzepte, Methoden und Anwendungen (pp.186-189). Weinheim, Germany: Psychologie-Verlags Union.
Emde, Robert N. & Fonagy, Peter (1997). An emerging culture for psychoanalytic research? International Journal of Psycho-Analysis, 78, 643-651.
Fichten, Wolfgang & Dreier, Birgit (2003). Triangulation der Subjektivität – Ein Werkstattbericht. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 4(2), Art. 29, http://nbn-resolving.de/urn:nbn:de:0114-fqs0302293 [Date of access: October 17, 2009].
Fiedler, Georg & Lindner, Reinhard (Eds.) (1999). "So hab ich doch was in mir, das Gefahr bringt." Perspektiven suizidalen Erlebens. Hamburger Beiträge zur Psychotherapie der Suizidalität, Vol. 1. Göttingen: Vandenhoeck & Ruprecht.
Fiedler, Georg; Altenhöfer, Astrid; Gans, Ilan; Gerisch, Benigna; Lindner, Reinhard & Götze, Paul (2007). Suizidalität und Psychotherapie. Das Hamburger Therapie-Zentrum für Suizidgefährdete. Suizidprophylaxe, 34(3), 113-122.
Fiedler, Georg; Götze, Paul; Gans, Ilan; Gerisch, Benigna; Lindner, Reinhard & Richter, Monika (1999). Psychoanalytische Psychotherapien bei akuter Suizidalität. Das Therapie-Zentrum für Suizidgefährdete in der ambulanten kassenärztlichen Versorgung Hamburgs – ein Überblick. Hamburger Ärzteblatt, 53, 537-542.
Fonagy, Peter (1996). The future of empirical psychoanalysis. British Journal of Psychotherapy, 12, 106-118.
Fonagy, Peter (Ed.) (1999). An open door review on outcome studies in psychoanalysis, a report prepared for the Research Committee of the London: International Psychoanalytical Association.
Freud, Sigmund (1914g). Weitere Ratschläge zur Technik der Psychoanalyse: II. Erinnern, Wiederholen und Durcharbeiten. In Sigmund Freud, GW, Vol. 10 (pp.125-136). Frankfurt/M.: Fischer.
Freud, Sigmund (1917e). Trauer und Melancholie. In Sigmund Freud, GW, Vol. 10 (pp.427-446). Frankfurt/M.: Fischer.
Froggett, L. & Briggs, S. (2009). Editorial Journal of Social Work Practice, Special Isssue on Practice-Near Research 4, 377-382.
Frommer, Jörg; Langenbach, Michael & Streeck, Ulrich (2004). Qualitative psychotherapy research in German-speaking countries. Psychotherapy Research, 14, 57-75.
Gerhardt, Uta (1990). Patient careers in end-stage renal failure. Social Science & Medicine, 30, 1211-1224.
Gerhardt, Uta (1991). Familiy rehabilitation and long-term survival in end-stage renal failure. Advances in Medical Sociology, 2, 205-244.
Gerhardt, Uta (1994a). The use of Weberian ideal-type methodology in qualitative data interpretation: An outline for ideal-type analysis. Bulletin de Méthodologie Sociologique, 45, 74-126.
Gerhardt, Uta (1994b). "Ideal type" and the construction of the life course. A new look at the micro-macro link. In Ansgar Weymann & Walter R. Heinz (Eds.), Society and biography (pp.21-50). Weinheim, specify country: Deutscher Studien Verlag.
Gerhardt, Uta (1999). Herz und Handlungsrationalität. Frankfurt/M.: Suhrkamp.
Gerhardt, Uta (2001). Idealtypus. Zur methodischen Begründung der modernen Soziologie Frankfurt/M.: Suhrkamp.
Gerisch, Benigna (1993). Aspekte zum psychodynamischen Verständnis der Suizidalität bei Frauen. Forum Psychoanalyse, 9, 198-213.
Gerisch, Benigna (1996). The unconscious motivation of suicidality among women. In Antoon A. Leenaars & David Lester (Eds.), Suicide and the unconcscious (pp.219-247). Northvale, New Jersey, London: Jason Aronson.
Gerisch, Benigna (1998). Suizidalität bei Frauen: Mythos und Realität; eine kritische Analyse. Tübingen, Germany: Edition diskord.
Gerisch, Benigna (1999). Wissenschaftstheoretische und psychoanalytische Aspekte zur weiblichen Suizidalität. Psychotherapie, 4, 156-163.
Gerisch, Benigna (2003). Die suizidale Frau. Psychoanalytische Hypothesen zur Genese. Göttingen, Germany: Vandenhoeck & Ruprecht.
Gerisch, Benigna; Fiedler, Georg; Gans, Ilan; Götze, Pal; Lindner, Reinhard & Richter, Monika (2000). "Ich sehe dieses Elendes kein Ende als das Grab": Zur psychoanalytischen Konzeption von Suizidalität und der Behandlung Suizidgefährdeter. In Gerd Kimmerle (Ed.), Zeichen des Todes in der psychoanalytischen Erfahrung (pp.9-64). Tübingen: Edition diskord.
Green, Andre (2000). Science und Science-Fiction in der Säuglingsforschung. Zeitschr für psychoanalytische Theorie und Praxis, 15, 438-466
Hagel, Markus (1995). Evidenz, Geltung und psychoanalytische Methode. In Erwin Kaiser (Eds.), Psychoanalytisches Wissen: Beiträge zur Forschungsmethodik (pp.72-91). Opladen, Germany: Westdeutscher Verlag.
Hale, Robert (2008). Psychoanalysis and suicide: Process and typology. In Stephen Briggs, Alessandra Lemma & Will Crouch (Eds.) Relating to self-harm and suicide: Psychoanalytic perspectives on theory, practice and prevention (pp.13-24). London: Routledge.
Harkness, Kate L. & Monroe, Scott M. (2002). Childhood adversity and the endogenous versus nonendogenous distinction in women with major depression. American Journal of Psychiatry, 159, 387-393.
Hawton, K., Zahl, D. & Weatherall, R. (2003). Suicide following deliberate self-harm: long-term follow up of patients who presented to a general hospital. British Journal of Psychiatry, 182, 537-542.
Hempel, Carl G. (1965). Fundamentals of taxonomy. In Carl G. Hempel (Ed.), Aspects of scientific explanation and other essays in the philosophy of science (pp.137-154). New York: Free Press.
Henseler, Heinz (1974). Narzisstische Krisen: Zur Psychodynamik des Selbstmords. Opladen: Westdeutscher Verlag.
Herzog, James (1980). Sleep disturbance and father hunger in 18 to 23-month-old boys. Psychoanalytical Study of the Child, 35, 219-233.
Herzog, James (1982). On father hunger: The father´s role in the modification of aggressive drive and fantasy. In Stanley H. Cath, Allan R. Gurwitt & John M. Ross (Eds.), Father and child (pp.163-174). Boston: Little, Brown and Company/or Co.
Hobson, R. P., Patrick.MP., Valentine, J.D. (1998). Objectivity in psychoanalytic judgements. The British Journal of Psychiatry, 173, 172-177.
Jacobs, Theodore J. (2000). Unbewusste Kommunikation und verdeckte Enactments im analytischen Setting. In Ulrich Streeck (Ed.), Erinnern, Agieren und Inszenieren (pp.97-126). Göttingen, Germany: Vandenhoeck & Ruprecht.
Joseph, Betty (1989). Psychic equilibrium and psychic change. London: Routledge.
Kandel, Erik R. (1998). A new intellectual framework for psychiatry. American Journal of Psychiatry (please confirm), 155, 457-469.
Kelle, Udo & Kluge, Susann (1999). Vom Einzelfall zum Typus: Fallvergleich und Fallkontrastierung in der qualitativen Sozialforschung. Opladen: Leske and Budrich.
Kind, Jürgen (1992). Suizidal. Psychoökonomie einer Suche. Göttingen, Germany: Vandenhoeck & Ruprecht.
Klein, Melanie (1957/1975). Envy and gratitude. In Melanie Klein, Envy and gratitude and other works (pp.176-235). London: Hogarth Press.
Klüwer, Rolf (2001). Szene, Handlungsdialog (Enactment) und Verstehen. In Werner Bohleber & Sibylle Drews (Eds.), Die Gegenwart der Psychoanalyse – die Psychoanalyse der Gegenwart (pp.347-357). Stuttgart: Klett-Cotta.
Kluge, Susann (1999). Empirisch begründete Typenbildung. Opladen: Leske and Budrich.
Kluge, Susann (2000). Empirically grounded construction of types and typologies in qualitative social research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 1(1), Art. 14, http://nbn-resolving.de/urn:nbn:de:0114-fqs0001145 [Date of access: October 17, 2009].
Laplanche, Jean & Pontalis, Jean-Bertrand (1972). Das Vokabular der Psychoanalyse. Frankfurt/M.: Suhrkamp.
Laufer, Moses & Laufer, M. Egle (1989). Adoleszenz und Entwicklungskrise. Stuttgart: Klett-Cotta.
Leuzinger-Bohleber, Marianne (1995). Die Einzelfallstudie als psychoanalytisches Forschungsinstrument. In Erwin Kaiser (Eds.), Psychoanalytisches Wissen: Beiträge zur Forschungsmethodik (pp.205-239). Opladen: Westdeutscher Verlag.
Leuzinger-Bohleber, Marianne (2002). Psychoanalytic research and the pluralism of sciences—some critical remarks. Presentation as Annual Research Lecture of the British Psychoanalytic Society, London, March 3, 2002.
Leuzinger-Bohleber, Marianne; Rüger, Bernhard; Stuhr, Ulrich & Beutel, Manfred (2002). "Forschen und Heilen" in der Psychoanalyse: Ergebnisse und Berichte aus Forschung und Praxis. Stuttgart: Kohlhammer.
Lindner, Reinhard (2003). Gegenübertragungsdiagnostik in der Psychotherapie suizidaler Männer. Psychotherapeut, 48, 230-239.
Lindner, Reinhard (2006). Suizidale Männer in der psychoanalytisch orientierten Psychotherapie. Eine systematische qualitative Studie. Gießen: Psychosozial-Verlag.
Lindner, Reinhard & Gerisch, Benigna (1997). "Wollten Sie wirklich sterben?" Zur Kontroverse psychiatrischer und psychodynamischer Aspekte der Suizidalität. Psychotherapie Forum, Suppl. 5, 65-68.
Lorenzer, Alfred (1973/2000). Sprachzerstörung und Rekonstruktion: Vorarbeiten zu einer Metatheorie der Psychoanalyse. Frankfurt/M.: Suhrkamp.
Mahler, Margret S., Pine, Fred, Bergman, Anni (1975). The psychological birth of the human infant. New York: Basis Books.
Malan David H. (1979). Individual psychotherapy and the science of psychodynamics. London: Tavistock.
Malterud, Kirsti (2001a). The art and science of clinical knowledge: Evidence beyond measures and numbers. The Lancet, 358, 397-400.
Malterud, Kirsti (2001b). Qualitative research: standards, challenges, and guidelines. The Lancet, 358, 483-488.
Maltsberger, John T. & Buie, Dan H. (1974). Countertransference hate in the treatment of suicidal patients. Archives of General Psychiatry, 30, 625-633.
Mayring, Philipp (2007). On generalization in qualitatively oriented research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 8(3), Art. 26, http://nbn-resolving.de/urn:nbn:de:0114-fqs0703262 [Date of access: October 17, 2009].
Menninger, Karl A. & Holzman, Phillip S. (1977). Theorie der psychoanalytischen Technik. Stuttgart: Frommann-Holzboog.
Meyer, Adolf-Ernst (1993). Nieder mit der Novelle als Psychoanalyse-Darstellung – Hoch lebe die Interaktionsgeschichte. In Ulrich Stuhr & Friedrich-Wilhelm Deneke (Eds.), Die Fallgeschichte: Beiträge zu ihrer Bedeutung als Forschungsinstrument (pp.61-84). Heidelberg: Asanger.
Perron, Roger (1999). Reflections on psychoanalytic research problems—the French-speaking view. In Peter Fonagy (Ed.), An open door review on outcome studies in psychoanalysis (pp.9-20). London: International Psychoanalytical Association.
Perron, Roger (2002). How far can we usefully develop clear criteria to assess psychoanalytic treatment and how do we set about it? Paper on the 3rd Joseph Sandler Research Conference, London, March 10, 2002.
Ratner, Carl (2002). Subjectivity and objectivity in qualitative methodology. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 3(3), Art. 16, http://nbn-resolving.de/urn:nbn:de:0114-fqs0203160 [Date of access: October 17, 2009].
Rosenfeld, Herbert A. (1987). Impasse and interpretation. Therapeutic and anti-therapeutic factors in the psychoanalytic treatment of psychotic, borderline and neurotic patients. London: Tavistock.
Rosenkötter, Lutz (1969). Über Kriterien der Wissenschaftlichkeit in der Psychoanalyse. Psyche, 23, 161-169.
Schwartz, Michael A. & Wiggins, Osborne P. (1987a). Diagnosis and ideal types: A contribution to psychiatric classification. Comprehensive Psychiatry, 28, 227-291.
Schwartz, Michael A. & Wiggins, Osborne P. (1987b). Typifications. The first step for clinical diagnosis in psychiatry. The Jounal of Nervous and Mental Diseases, 175, 65-77.
Stuhr, Ulrich (1995). Die Fallgeschichte als Forschungsmittel im psychoanalytischen Diskurs – Ein Beitrag zum Verstehen als Methode. In Erwin Kaiser (Ed.), Psychoanalytisches Wissen: Beiträge zur Forschungsmethodik (pp.188-204). Opladen: Westdeutscher Verlag.
Stuhr, Ulrich (1997). Psychoanalyse und qualitative Psychotherapieforschung. In Marianne Leuzinger-Bohleber & Ulrich Stuhr, (Eds.), Psychoanalysen im Rückblick: Methoden, Ergebnisse und Perspektiven der neueren Katamneseforschung (pp.164-181). Gießen: Psychosozial-Verlag.
Stuhr, Ulrich (2001). Methodische Überlegungen zur Kombination qualitativer und quantitativer Methoden in der psychoanalytischen Katamneseforschung und Hinweise zu ihrer Integration. Oder: Rhetorische Sprachfiguren als Stolpersteine auf dem Weg zur Einheitswissenschaft. In Ulrich Stuhr, Marianne Leuzinger-Bohleber & Manfred Beutel (Eds.), Langzeit-Psychotherapie: Perspektiven für Therapeuten und Wissenschaftler (pp.133-148). Stuttgart: Kohlhammer.
Stuhr, Ulrich & Wachholz, Sylvia (2001). In search for a psychoanalytic research strategy: The concept of ideal types. In Jörg Frommer & David L.Rennie (Eds.), Qualitative psychotherapy research—Methods and methodology (pp.153-169). Lengerich: Pabst Science Publishers.
Stuhr, Ulrich; Höppner-Deymann, Sigrid & Oppermann, Matthias (2002). Zur Kombination qualitativer und quantitativer Daten – "Was nur erzählt werden kann". In Marianne Leuzinger-Bohleber, Bernhard Rüger, Ulrich Stuhr & Manfred Beutel (Eds.), "Forschen und Heilen" in der Psychoanalyse: Ergebnisse und Berichte aus Forschung und Praxis (pp.154-179). Stuttgart: Kohlhammer.
Stuhr, Ulrich; Lamparter, Ulrich; Deneke, Friedrich-Wilhelm; Oppermann, Matthias; Höppner-Deymann, Sigrid; Bühring, Brigitte & Trukenmüller, Michael (2001). Das Selbstkonzept von "Gesunden". Verstehende Typenbildung von Laien-Konzepten sich gesundfühlender Menschen. Psychotherapie & Sozialwissenschaft, 3, 98-118.
Wachholz, Sylvia & Stuhr, Ulrich (1999). The concept of ideal types in psychoanalytic follow-up research. Psychotherapy Research, 9, 327-341.
Walkerdine, Valerie; Lucey, Helen & Melody, June (2002). Subjectivity and qualitative method. In Tim May (Ed.), Qualitative research in action (pp.179-196). London: Sage.
Wallerstein, Robert S. & Sampson, Harold (1997). Wichtige Fragen der psychoanalytischen Prozeßforschung. In Stefan de Schill, Serge Lebovici & Horst Kächele, (Eds.), Psychoanalyse und Psychotherapie: Herausforderungen und Lösungen für die Zukunft (pp.132-154). Stuttgart: Thieme.
Webb, Eugene J.; Campbell, Donald T.; Schwartz, Richard D. & Sechrest, Lee (1975). Nicht-Reaktive Meßverfahren. Weinheim: Beltz Verlag.
Westmeyer, Hans (1979). Die rationale Rekonstruktion einiger Aspekte psychologischer Praxis. In Hans Albert & Kurt H. Stapf (Eds.), Theorie und Erfahrung (pp.139-161). Stuttgart: Klett-Cotta.
Weber, Max (1904/1988). Die "Objektivität" sozialwissenschaftlicher und sozialpolitischer Erkenntnis. In Max Weber, Gesammelte Aufsätze zur Wissenschaftslehre (pp.146-214). Tübingen: Mohr.
Williams, Malcolm (2006). Generalize double check spelling since it was published in Londonation in interpretive research. In Tim May (Ed.), Qualitative research in action (pp.125-143). London: Sage.
Winnicott, Donald W. (1965). Maturational processes and the facilitating environment. London: Hogarth Press.
Wolff, Peter H. (1996). The irrelevance of infant observation for psychoanalysis. Journal of the American Psychoanalytical Association, 44, 369-473.
Reinhard LINDNER, Privatdozent Dr. med., Specialist in Neurology, Psychiatry, Psychotherapy and Psychosomatic Medicine, Head of the Center for Therapy and Studies of Suicidal Behavior, University Hospital Hamburg-Eppendorf and, with a scholarship of the Forschungskolleg Geriatrie, Robert Bosch Foundation, Stuttgart, Psychosomatic Consultant at the Centre for Geriatrics and Gerontology Albertinen-Haus, Hamburg.
Contact:
Reinhard Lindner
Therapie-Zentrum für Suizidgefährdete
Universitätsklinikum Hamburg-Eppendorf
Martinistr. 52
20246 Hamburg, Germany
E-mail: lindner@uke.uni-hamburg.de
Stephen BRIGGS, PhD, Associate Dean, Specialist and Mental HealthServices, Tavistock and Portman NHS Foundation Trust, London and Professor of Social Work, Director of the Centre for Social Work Research, School of Humanities and Social Sciences, University of East London.
Contact:
Stephen Briggs
Adolescent Department
Tavistock Clinic
London NW3 4BA, UK
E-mail: SBriggs@tavi-port.nhs.uk
Lindner, Reinhard & Briggs, Stephen (2010). Forming Ideal Types by Understanding: The Psychoanalytic Treatment of Suicidal Men [65 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 11(2), Art. 12, http://nbn-resolving.de/urn:nbn:de:0114-fqs1002120.

Creative Commons Attribution 4.0 International License