Volume 10, No. 2, Art. 5 – May 2009
An Integrity Perspective on the Decentralization of the Health Sector in Colombia
Gloria Molina M.
Abstract: This study analyzes the decentralization of the health sector in Colombia by exploring the characteristics of Institutional Development and Community Participation and their relationship with the socio-economic conditions of Colombian municipalities, as well as the administrative and political issues that affect the implementation processes at the municipal level. The analysis is framed in the context of health sector reform, and decentralization is understood as a public policy which interacts strongly with the political, social, economic and administrative environments. The methodology involves qualitative and quantitative methods; three case studies and a survey of 91 municipalities were carried out. The findings from different sources and methods suggest that the level of progress in the health sector is not consistent with the socio-economic categories in which the municipalities have been classified. This is closely related to the quality of the staff working within the health sector, which is, in turn, connected with the patronage system and the political will of the municipal, regional and national governments.
Key words: mixed methods; qualitative study; quantitative study; health sector reform; institutional development; community participation; Colombia
Table of Contents
1. Introduction
2. Main Theoretical Concepts
2.1 Relationship between political parties and the state in Colombia
2.2 The Neo-liberal model and the health sector reform
3. Methodology
4. Results
4.1 Relationship between political issues, administrative capacity and autonomy of the municipalities
4.1.1 Fluctuation or lack of political will in supporting decentralization
4.1.2 Quality of the staff as linked to the political patronage system
4.1.3 Limited development of key administrative processes
4.1.4 Poor institutional capacity and autonomy of health entities
4.2 Tensions between private and public entities in the provision of health services
4.2.1 Imbalance in the geographical distribution and development of the health infrastructure
4.2.2 Limitation in provision of services
4.3 The limited role of national and provincial health authorities
4.4 The underdevelopment of Community Participation (CP)
5. Discussion
Colombia is located in northwest South America. In 2000, the population was estimated at 42,299,301, comprising 49.5% males and 50.5% females. The urban population represents 75% of the total, and the rural population 25% (THE WORLD BANK, 2001). The country is divided in 32 departments (or provinces) which, in 2000, had 1,080 municipalities classified into 7 categories (E and from 1 to 6) according to their socio-economic development (Law 60, 1993; Law 715, 2001)1). The most developed municipalities are the largest cities of Bogotá, Medellín and Cali, which are in category E (representing 0.5% of the total number of municipalities); the other biggest cities are in category 1 (1.5%) and 2 (2.8%). The middle size municipalities are in categories 3 (5.4%) or 4 (11.5%) and the smallest and poorest municipalities are in categories 5 (32.4%) or 6 (46.2) (ASOCIACIÓN NACIONAL DE SECRETARÍAS MUNICIAPALES DE SALUD, 2000). [1]
Decentralization has been seen as an appropriate policy to improve the efficiency and effectiveness or impact of the programs carried out by the state, increasing coverage, accessibility and quality of the public services. The first municipal and regional elections took place in 1988. Legislation has been issued to transfer the central government’s responsibilities to the municipal and departmental governments, such as the Law 10 of 1990. Also, the Law 60 of 1993 and the Law 715 of 2001 introduced a fiscal reform and allocated resources for the health sector. Law 100 of 1993 on Social Security for Health introduced a wider and deeper reform of the health sector, created new organizations and new ways to obtain resources and assigned new responsibilities to municipalities. Decentralization of the health sector has also been introduced in other Latin American countries such as Chile, Brazil, Bolivia and Argentina (BURKI, PERRY & DILLINGER, 1999; COLLINS, ARAUJO & BARBOSA, 2000). This is in line with international economic forces and health policies, which have demanded that governments, in both developed and developing countries, carry out health sector reforms (BLOOM, 2001; ISLAM & TAHIR, 2002; LEGEMAATE, 2002; SEN, 2000; THE WORLD BANK, 1993). [2]
Some empirical studies have analyzed various aspects of the health sector, and/or of the reform of the state in Colombia: a) decentralization of the state and local governments (ANGELL, LOWDEN & THORP, 2001; THE WORLD BANK, 1995); b) changes in the origin of health financial resources (DEPARTAMENTO NACIONAL DE PLANEACION, 1999); c) decentralization of the health sector (LA FORGIA & HOMEDES, 1992; THE WORLD BANK, 1995); d) health human resources (SUPERINTENDENCIA NACIONAL DE SALUD, 1995; e) community and citizen participation (FORERO, HIDALGO & JIMENEZ, 1997; MOSQUERA, ZAPATA, LEE, ARANGO & VARELA, 2001), and f) the social security system (for Health) (CARDONA, ARBELAEZ & CHAVEZ, 1999; CASTAÑO, ARBELAEZ, GIEDION & MORALES, 2001; FERNÁNDEZ & PASTOR, 2001; PLAZA, BARONA & HEARST, 2001; SILVA, HERRERA & AGUDELO, 2002); but no study has provided an integrated analysis of Institutional Development (ID) and Community Participation (CP) yet. [3]
This study explores the characteristics of ID and CP in municipalities according to the category in which they have been classified, the interaction of the different constituents of ID and CP and the political and administrative factors that have affected the implementation of decentralization in the health sector since 1993. Both quantitative and qualitative methods were used. The main findings showed that the implementation of different aspects of ID and CP has made a moderate amount of progress, which is neither integrated nor consistent with the categories in which these municipalities have been placed. There is a relationship between the political and administrative issues involved in the decentralization process, within which the political will of government, the political patronage and the quality of the staff are related to the progress of the decentralization process. [4]
2.1 Relationship between political parties and the state in Colombia
The Modern State is based on the achievement of the values of liberty, justice, equity and solidarity, which are closely connected with social and individual well-being and autonomy (NIETO, 1997, p.53). The historic period of the Republic in the 19th century demanded the existence of a Nation2) that implied or required the values of the Modern State (ZAMBRANO, 1989). Historically, in Colombia, the Creole elite created the Nation and the State, based on a political culture characterized by a combination of political parties (politicians that belonged to the conservative and liberal political parties) and religious groups. The dominant elite and its political parties defined and organized the state and its institutions according to their interests along a top-down hierarchy (ARRUBLA, 1991). The role of political parties in a society may be understood along with the development of the state. They have three principal functions: a) to articulate and add interests, b) to define political alternatives and c) to generate ideologies and utopias (VILLA, 1997). However, in Colombia, as in other Latin American countries, political parties appear to be mainly electoral machines that branch out from the state and, therefore, are not independent from it, a condition that serves as a foundation for the patronage system. In addition, representative democracy has dominated the political system in Colombia, within which electoral issues fragmentize social groups, leading to a limited development of citizenship and civil society (VILLA, 1997). In this context, affiliation to a specific political party allows some individuals to obtain jobs or subsidies for education and health, which facilitates/perpetuates the operation of the patronage system. [5]
2.2 The Neo-liberal model and the health sector reform
The Welfare State model is based on KEYNES' theories.3) It was introduced as a means to build a new society that allowed modern values to reappear with the idea of infinite progress, and to enable European countries to recover from the destruction caused by the First and Second World Wars. SUNKEL (2006) points out that, within the welfare model, the state has economic, social and political functions, and that public investment allows for the development of public services on a large-scale model, covering all citizens. But, in Latin American countries, the Welfare State did not achieve sufficient development, and the state was unable to satisfy the growing/increasing needs of the population. [6]
The Neo-liberal4) model was mainly introduced in developing countries in the 1980s and 1990s as part of the Structural Adjustment Programs demanded by the World Bank and the International Monetary Fund. The model is based on the New Right Perspective,5) which supports the argument that reducing the role of the state as the main provider of public services will solve the economic, social and political problems created by the Welfare State. State provision should be aimed at those who have no resources or any other sources of support (NORTH & BRADSHAW, 1997; BURDEN et al., 2000). The key tenets of the neo-liberal strand are as follows: minimal state intervention, increasing role of the private sector, freedom, individual choice and free market. Market is considered as the means to generate goods and services more efficiently and to guarantee individual freedom. As Neo-liberalism strengthens a minimal state, individuals must be responsible for satisfying their needs. [7]
The health sector reforms introduced in developing countries in the 1990s are based on Neo-liberalism. They have emphasized market, privatization of care provisions and moved responsibilities for financing services from the government to users (BENNETT, McPAKE & MILLS, 1997; COLLINS, GREEN & HUNTER, 1999; EXWORTHY & HALFORD, 2002; NORTH & BRADSHAW, 1997; VEGA, 2001). ISLAM and TAHIR (2002, p.152) also highlight the fact that "in many developing countries, social sector reform is dictated more by donor agencies, rather than by any national rational decision." Therefore, these reforms often do not take into account specific social, cultural, economic, demographic and epidemiological contexts, which has serious impacts on the health sector. [8]
The New Public Management approach was introduced as part of the state and health sector reforms; this approach also emphasizes the decentralization, managerialism, efficiency, and privatization of public institutions as means to increase the effectiveness of public institutions. Within the context of decentralization, municipalities are seen as privileged spaces within which democracy and sustainable development are obtained through a larger participation of the community (VELÁSQUEZ, 1996). [9]
Decentralization is understood as a public policy, which is part of a wider reform of the state and the health sector; it seeks to improve the accessibility, efficiency, effectiveness, equity and quality of health services. A public policy is a governmental action; it is whatever a government chooses to do or not to do (DYE, 1972; ROTH, 2006). It is a purposive course of actions that one or several actors follow in order to deal with a problem. It generates a web of interrelations among different activities, sectors and organizations (HILL, 1997; VARGAS, 1999); therefore, its implementation is complex and requires participation, co-ordination and negotiation among the actors involved (AYEE, 1994; HOGWOOD & GUNN, 1997; POWELL, 1999; WALT, 1994). PRESSMAN and WILDAVSKY (1984) define the implementation of public policies as the ability to forge subsequent links in order to obtain the desired results in the causal chain. The longer and more complex the chain of causality is, the more numerous the reciprocal relationships among the links develop and the more complex the implementation process becomes. Decentralization involves an allocation of political power, resources, decision-making and management functions from the central government to such bodies as field agencies, subordinate units of government, semi-autonomous public corporations, local government and community organizations (BANKAUSKAITE & SALTMAN, 2007; LÓPEZ, 1995; RONDINELLI, 1990). [10]
In order to implement decentralization, the sub-national levels should build and/or strengthen ID and mechanisms for CP. ID involves the creation and the strengthening of capacity within institutions and/or organizations to generate, assign and use resources efficiently and effectively in order to accomplish the objectives (MONTIEL, 1998). CP is a complex process linked to the democratization process, to cultural values and to the political, economic and social contexts. It involves the profound and continuous education of both individuals and the community on collective values as the foundations of society, which could support CP as a process through which the community participates in the planning of the implementation of public policies or programs, evaluation of and decision-making on public issues (that affect the individuals and the community) (MULLER, 1991; PENAGOS, 1994; THE WORLD BANK, 1995). [11]
Based on the theoretical concepts of ID and CP, and on the Colombian legislation, an analytical framework was set up. ID includes several factors such as the analysis of the effectiveness of health sector administrative entities at the municipal level, the planning process and management of human resources, the Health Information System (HIS), the health infrastructure and supply of services, the quality assurance system and the surveillance and control system. CP includes the number and types of community organizations involved in health issues, the role of these organizations in influencing decision-making on health, as well as the aspects that affect their participation. [12]
The analysis of these dimensions required the definition of variables, which were used as a basis for designing a structured questionnaire (OPPENHEIM, 1992); a semi-structured guide for interviews was also designed (see Appendix 1) in order to gather information from key informants (BOURQUE & FIELDER, 1995; BRYMAN, 1988; MULLEN & SPURGEON, 2000). Pilot tests of these instruments were conducted in order to ensure their validity and reliability (KEPPEL & ZEDECK, 1989). [13]
This study allowed for an integrated analysis of the decentralization of the health sector using both quantitative and qualitative approaches (MILES & HUBERMAN, 1994; PATTON, 1997; PUNCH, 1998). The quantitative analysis involved a survey of municipalities from three provinces: Antioquia, Caldas and Risaralda, which share similarities in terms of their cultural, economic, political and administrative contexts. The qualitative study included three municipalities, selected as case studies (STAKE, 1994; YIN, 1994): Municipality A (MA), Municipality B (MB) and Municipality C (MC),6) classified in categories 1, 4 and 6, respectively. Information was gathered through individual semi-structured interviews (FLICK, 1998; MAY, 1997) and focus groups (DREACHSLIN, 1998; MORSE, 1994; MULLEN & SPURGEON, 2000). A group of decision-makers from the municipal, provincial and national levels was selected as a purposive sample (GLASER & STRAUSS 1967; MILES & HUBERMAN, 1994; SILVERMAN, 2000). The participants were contacted by phone and informed about the purpose of the research in order to get their consent to participate in the study and make arrangements for appointments. Confidentiality of information and identification were guaranteed to all participants. Ethical issues were supervised by the Committee of Ethics of the Universidad de Antioquia Research Center. This study was also supported by the Pan American Health Organization. Thus, 17 key informants were interviewed at the municipal level: mayors, municipal health directors, directors of public and private hospitals, heads of health insurance companies and people/staff/officers from the municipal planning office. Additionally, six focus groups were carried out, in which 44 representatives of the community participated. In addition, and in order to include the perspectives of national and provincial health authorities, 14 decision-makers were interviewed: 5 from the Ministry of Health, 1 from the National Planning Office, and 8 from the Regional Health Authorities of Antioquia, Caldas and Risaralda. The analysis of qualitative data implied the transcription of the interviews and the coding process in order to identify categories (GLASER & STRAUSS, 1967; MILES & HUBERMAN, 1994; STRAUSS & CORBIN, 1990). 1,094 codes related to ID and CP were generated, out of which 27 descriptive categories and 4 analytical categories emerged. [14]
The quantitative study involved a survey of municipalities, for which a self-completed questionnaire was sent by mail to 164 municipalities, of which 91 (55.5%) responded to the questionnaire. These municipalities belong to different categories (1: 5.5%; 2: 4.4%; 3: 3.3%; 4: 15.4%; 5: 33% and 6: 38.5%); this percentage is consistent with the proportion of municipalities in these regions. 85.1% of the respondents were Municipal Health Directors (MHD), and the remaining 14.9% were mayors. Data analysis included a descriptive statistical analysis, a Principal Component Analysis (PCA), and a correlation analysis. The PCA of the survey of municipalities generated 10 Principal Components, which represent 65.45% of the accumulated variance. [15]
The process of combining the research methods, sources of information and findings was intended to strengthen the validity and reliability of this study (CRESWELL & PLANO CLARK, 2007; GREENE & CARACELLI, 2003; MILES & HUBERMAN, 1994); and in this particular case, it allows for an integrated comprehension of the decentralization process. [16]
This article presents the major findings on ID and CP obtained from the three sources used for the investigation (the case studies, the interviews with regional and national decision-makers, and the survey); in addition, the categories obtained through/emerging from the qualitative analysis are highlighted. Only part of the results obtained from the survey are included in order to change verb, I don’t see what you mean here the findings and provide further argumentation—and a more thorough understanding—of some the most relevant aspects of this study. Thus, four analytical categories are presented below. [17]
4.1 Relationship between political issues, administrative capacity and autonomy of the municipalities
Findings from the three sources are consistent in terms of the municipalities' political and administrative areas, which have been closely related to the decentralization of the health sector. In the political field, there are two relevant components: fluctuation in or lack of political will (and therefore lack of continuity in the decentralization process) and a political patronage that affects the quality of the staff, which in turn affects the development of basic administrative processes, such as planning, the health information system, and the surveillance and monitoring system (see Figure 1).
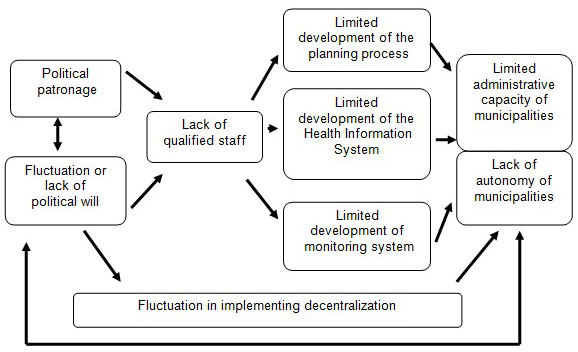
Figure 1: Relationship between political issues, technical capacity and autonomy of the municipalities [18]
4.1.1 Fluctuation or lack of political will in supporting decentralization
In the Colombian political system, municipal mayors and provincial governors are elected every three years, and the president every four years. This means that staff, and especially the decision-makers of the public, and even of some private institutions, are regularly removed from office and that new staff are appointed instead. The rulers establish their own agenda, in which the decentralization process does not appear as a priority; on the contrary, the political groups are more interested in supporting those policies and programs, from which they can derive benefit. Decentralization implies a strong political, social and economic commitment of the groups in power, but not all of them assume such a commitment. Lack of political support for decentralization generates a lack of continuity in its implementation, since the administrative processes put in place by one government are generally not continued by the next one, and that all the efforts and resources invested are eventually lost. The following codes give support to these concepts:
"The poor commitment of the rulings in addressing the work of health in the municipality and the lack of political will have limited the organization of the health sector" (EI-1).
"In the municipality B, the lack of political will to organize the health sector, frequent changes of health top-managers and the lack of continuity of policies have been very important factors in preventing the development of the health sector. For instance, the health secretary was changed four times within the last year as a consequence of political influence" (EC-1).
"The municipal health staff is dismissed very often. Some staff is changed every six months, for instance the co-coordinators of the Basic Health Plan. There is no continuity in the process" (EC-1).
"When a new municipal government starts, all the municipal secretaries are dismissed and new ones are appointed, without bearing in mind the projects that they were carrying out, which is not good especially for some public sectors such as health and education" (EI-1). [19]
4.1.2 Quality of the staff as linked to the political patronage system
Historically, the Colombian political parties have been in close relationship with the development of the state and with its public institutions, which are even said to exist not for the community but for political parties. Rulers promise jobs to their followers in order to get their votes. This dynamics creates a political patronage system—or clientelism—which affects the institutional capacity to lead public health policies and programs and also contributes to corruption. In this context, every three or four years, rulers change and, therefore, those who get votes for the political leaders are offered positions in the administrative level of public institutions. In general, the people appointed to public institutions positions do not have any technical or professional qualification for the jobs. Moreover, the mayors of many municipalities have a very low professional training. The case studies showed that the MHD's do not usually count on sufficient personnel to carry out the functions of this entity. There is also a constant turnover of the staff deriving from the political patronage system. The survey showed that 81.3% of the municipalities had a Municipal Health Director who was responsible for the sector. However, 40.5% of these directors and 60% of the whole MHD staff did not have the appropriate qualifications for carrying out their functions; and 65% of them had been working for the MHD for less than one year only. The number of staff qualified on key issues of public health, such as epidemiology and health information systems, was insufficient. The three case studies showed a decline in the staff of public hospitals and health centers, such as nurses, dental hygienists, dentists and rural health promoters, whose services are provided specifically in the area of preventive care. The perspective of national and regional decision-makers suggests that the lack of skilled staff and its high turnover rate have affected the effectiveness of the technical assistance and, therefore, of the administrative capacity of health authorities. Some codes of the interviews support these findings
"... We cannot deny that this is a political country, in which whoever wins power also wins the opportunity to appoint staff in the public organizations" (EI-1).
"The operation of the MHD has been affected by the uncertainty of officials from the MHD and their academic profile with little technical emphasis, but a greater patronage one. Little importance has been assigned to the administration of the health on the part of the municipal government" (EC-3).
"The municipal government had managed the MHD with a lot of political clientelism, therefore people have not had professional training for that position" (EB2).
"Most of the Municipal Health Secretaries have not been able to understand the process of decentralization of the health sector" (EC-3).
"The staff from disciplines other than health, without training in health issues, has made the implementation of decentralization more difficult" (ER-1).
"Some municipal health secretaries do not have an appropriate academic profile for this post; e.g. one of them is trained in agricultural issues, but not in health" (EC-1). [20]
4.1.3 Limited development of key administrative processes
A consequence of the lack of sufficient and qualified staff is a limited development of the following key administrative processes involving the following constituents: [21]
a) The Health Information System (HIS), which demands coordination between health institutions in order to manage a complex network of inter-institutional relationships for the gathering of data. The case studies showed that the smallest municipality, MC, showed better quality and a greater effectiveness of its HIS than MA and MB. From the perspective of national and regional decision-makers, frequent changes in HIS regulations issued by the Ministry of Health, along with the lack of technological infrastructure of the municipalities, have limited the development of the HIS, which has affected the whole management process. This code from interviews supports this finding:
"The problem nowadays is that we do not know the population's coverage because the previous information system was stopped and the new one has not been implemented. The previous one provided at least basic indicators, but nowadays many activities are carried out but their effectiveness is not known" (EII-1). [22]
Additionally, the survey shows that the quality of information was poor or moderate in most types of municipality, and that the quality of some types of information was even better in municipalities in categories 5 and 6 than in those in categories 1 and 3. The effectiveness of information in terms of decision-making was similar (moderately or effective) in all types of municipality. The Principal Component Analysis (PCA) shows that the quality and effectiveness of HIS are essential factors of decentralization. Thus, its quality is associated with the effectiveness of decentralization to improve the accessibility to health services (p=0.003) and with the level of progress of the decentralization process (p=0.009). [23]
b) The planning process, which demands qualified staff able to obtain and use information and knowledge in order to analyze the community's health situation, foresee future events and establish the appropriate strategies to tackle health problems. The case studies demonstrated that the planning process is still weak; however, MA has progressed in implementing this process further than MB and MC. The perspective of national and departmental decision-makers suggests that the planning process has made limited progress, due to the lack of an appropriate and qualified HIS staff. In addition, findings from the survey of municipalities suggest that the planning process has developed further in municipalities in categories 1 and 2 than in those in categories 3, 4, 5 and 6.
"In the MHD there is no cross-sectoral and inter-institutional teamwork referred to health planning" (EC-5).
"The lack of political and administrative will of the municipal administration did not allow the development of the MHD" (EB1). [24]
c) The surveillance and monitoring system, which is an administrative process that requires staff with large experience within the health sector. The case studies found that MA had made a little more progress in surveillance and monitoring than MB, but in both municipalities the effectiveness has been very limited. In MC there has not been any surveillance in health. The findings related to surveillance and monitoring systems of the health sector reveal that the state has lost power, and that national, provincial and municipal health authorities have not been able to carry out effective surveillance and monitoring processes of all the actors involved in the health sector. Their role has been very limited in controlling the private Health Promoter Enterprises (HPEs) and Subsidy Scheme Administrators (SSAs), which have not fulfilled the principles established in the legislation for the provision of services. Also, the survey of municipalities showed that, in spite of the fact that 86.9% of the municipalities have implemented the financial audit process, its effectiveness is still limited. Likewise, the national and provincial entities, which carry out surveillance and monitoring, were rated as moderately effective or ineffective in all types of municipality. These codes illustrate the findings:
"Surveillance and control are very limited in the municipality and even in the entire health system" (EII-2).
"I do not know any activity carried out by the entities that should do surveillance and control of the health system" (EILC-1).
"The National Superintendent of Health is not able to control the private sector and deal with complaints from users and from other organizations, because everybody is in Bogotá. It is very centralized" (EII-3). [25]
4.1.4 Poor institutional capacity and autonomy of health entities
Political issues and administrative processes are the bases for building institutional capacity, which in turn is the foundation of autonomy. The perspective of national and regional decision-makers suggests that, in spite of the fact that the municipalities have progressed in implementing some administrative processes, they have not been sufficiently effective in accomplishing all of their functions related to the health sector. Limited administrative capacity and lack of autonomy in turn facilitates political patronage (see Figure 1). [26]
In coherence with qualitative findings, the survey showed similar levels of municipal effectiveness (index of 3.2-3.5) in accomplishing their functions of the following entities: Municipal Health Directorate (MHD), Municipal Health Fund (MHF), Health Promoter Enterprises (HPEs) and Subsidy Scheme Administrators (SSAs). The Municipal Council of Social Security for Health (MCSSH) was created in only 10% of the municipalities.
"There is a lack of institutional capacity of the municipalities to assume the functions allocated" (IN-P).
"The municipalities have created the municipal health secretary and the municipal health fund, but there is a lack of capacity for controlling the sector" (ER-3).
"There is no municipal capacity to tackle decentralization" (EC-2).
"There have not been coherent and integrated strategies in political, administrative and financial aspects of the decentralization process" (EA-2). [27]
4.2 Tensions between private and public entities in the provision of health services
Improving quality and accessibility of health services is the goal of health decentralization. However, findings suggest that this has been affected by several aspects (see Figure 2):
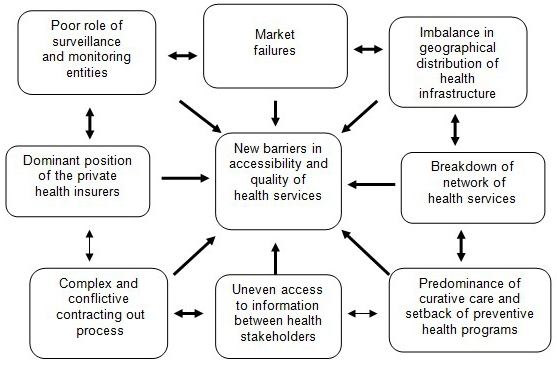
Figure 2: Tensions in the provision of services [28]
4.2.1 Imbalance in the geographical distribution and development of the health infrastructure
As decentralization has been introduced along with privatization, in MA and MB the number of private hospitals and health centers has increased, and also the public hospitals have improved their infrastructure to provide curative care, while in the three municipalities the provision of preventive programs has been reduced. The survey showed that the biggest and richest municipalities (categories E, 1 and 2) have more health infrastructure, also the private providers have increased and are concentrated in these type of municipalities; on the contrary, the public sector is the most important provider in the smallest and poorest municipalities. [29]
4.2.2 Limitation in provision of services
Municipalities are in charge of allocating subsidies to the poorest, for which a system for targeting the population, called SISBEN,7) is used. Most municipalities (87.9%) have covered more than 70% of the population with SISBEN. However, the case studies revealed that SISBEN has failed in several areas: the database has not been updated on time, there has been political manipulation, and some people have been incorrectly classified as poor. In addition, the findings from the survey and case studies suggest that, out of all the types of municipality, 79.1% have had two or more HPEs and SSAs, and municipalities in categories 1, 2, 3 and 4 have several health institutions. However, the HPEs and SSAs in charge of managing the subsidy scheme are selected by mayors and therefore, in practice, the population affiliated to them has limited opportunity to choose their insurance company and hospitals. Findings also revealed that more population is affiliated to the insurance system, which is expected to enable the poorest in the subsidy scheme to gain easier access to health services. However, effective accessibility to health services of good quality has been affected by several problems: private insurers have achieved a dominant position and have generated market failures; unfair competition and conflicts among stakeholders linked to the contracting process; the fragmentation of services; the imbalance in distribution of health infrastructure; the breakdown of the network of services; the predominance of curative care to the detriment of preventive programs; the poor role of surveillance and monitoring entities, and higher administrative costs (see Figure 2). Some codes from interviews illustrate these problems:
"The private intermediaries are given the direction to the health system and more especially to the subsidy scheme; they have appropriated the health resources. They influence and manage the market and in practice define policies. The state has disappeared; mayors are a ‘zero on the left' to control the lucrative interests of the private intermediaries, who are untouchable" (EA-1).
"Private intermediary companies are unnecessary to manage the subsidy scheme. This policy has permitted private intermediaries to enrich themselves at the expense of health resources" (ER-1). [30]
The following are examples of the difficulties that affect the accessibility and quality of services:
Some HPEs, especially the private ones, have not provided health services in the municipalities where their affiliated population is located; they have contracts for primary care services with health institutions from other municipalities in order to get lower prices. Therefore, patients have to go to hospitals in other municipalities, which increases costs for them and creates geographical barriers in accessing health services.8)
There are difficulties in the contracts between purchasers (HPEs and SSAs) and providers (hospitals and health centers). The HPEs and SSAs play a dominant role and do not renew the contracts on a timely basis, so hospitals cannot provide services when users request them.
HPEs and SSAs have not paid the bills to the providers promptly, which has generated financial problems or a collapse in the public hospitals.9)
Some providers have made contracts with HPEs and SSAs based on prices lower than the actual costs in order to survive financially in the short term. This generates unfair competition and financial risks in the sustainability of all the providers in the middle and the long term.
Linked to the contracting problems, the provision of services has been fragmented,10) due to the separation of preventive care and curative care, and a wide scale introduction of contracts among health organizations. Therefore, patients have to go to different health organizations to receive basic services: a medical consultation in an organization, clinical tests in another, and X-rays or medicines prescribed by a doctor in yet others. [31]
These codes from interviews support the findings:
"Not all the Health Promoters Enterprises contract services in the hospitals and health centers of the municipality. Many times patients have to look for services in other municipalities or in the biggest cities" (EIB-2).
"The Health Promoters Enterprises make contracts with hospitals from other municipalities to get low prices. They do not contract with the hospitals of this municipality. They do not use the infrastructure that the municipality has, which is not very good" (EILC-4).
"The SSAs and HPEs do not pay bills on time to the public hospitals, leading to their financial collapse. They manipulate the negotiation of contracts and pay services to hospitals based on tariffs which undercut the costs" (EA-2).
"The fragmentation and lack of integrity of health services have decreased the quality of services" (EILC-3). [32]
Limitations in the provision of services are linked to the administrative capacity of each municipality. The findings from the survey suggest that the effectiveness of decentralization in improving accessibility to health services is associated with the high administrative capacity of the municipalities (p = 0.008) and the good quality of the information system (p = 0.003). [33]
4.3 The limited role of national and provincial health authorities
The decentralization of the health sector is part of a wider reform of the state, focused on the reduction of public expenditure. In this context the staff of the Ministry of Health and the Provincial Health Department in Colombia has been reduced significantly, and municipalities must be in charge of managing the health sector. As pointed out above, the national and provincial levels are affected by the patronage system, and, therefore, there has been a lack of qualified personnel, which limits their capacity to lead the sector and carry out technical assistance to municipalities. At the same time, there has been an overloaded and complex legislation on decentralization, and the Social Security System for Health has experienced a lack of coordination among the health authorities at different levels of government. All these aspects have contributed negatively to the achievement of institutional capacity and autonomy of the municipalities (see Figure 3).
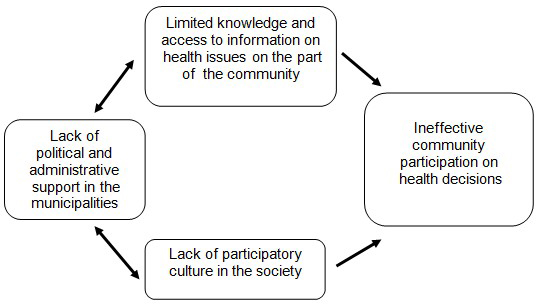
Figure 3: Underdevelopment of community participation [34]
The following codes give support to these concepts:
"Some programs of technical assistance have only been theoretical papers than practical applications to the municipalities" (EM-3).
"Technical assistance should be much more than conferences and papers. It should include appropriate learning methods, not only handbooks" (EM-1).
"The office of Ministry of Health that has provided technical assistance to decentralization has been reduced progressively. Nowadays, there are only 5 professionals to support to the whole country; which, in practice, is impossible" (EM-3).
"The decentralization process requires co-ordination between different levels of government" (EM-3).
"There has been very limited co-ordination of activities between different actors involved within the health sector" (ENP). [35]
4.4 The underdevelopment of Community Participation (CP)
The Colombian government issued a legal framework to organize CP, involving the creation of specific community organizations to carry out activities related to health issues, as well as the allocation of new functions to community organizations already in existence. Findings showed that the most numerous and representative organizations in the municipalities are the Communal Action Boards (CABs); the legislation encouraged the creation of one CAB in each urban neighborhood and rural village. But user associations and citizens watchdogs have had limited development. The survey and case studies revealed that these community organizations have not been effective enough in decision-making on health issues (indices of 1.5-2.0). The representatives of these organizations have not been able to access sufficient training, information and infrastructure (such as an office, a phone line and transportation) to participate effectively. The findings also suggest that there is a lack of participatory culture, and the large legal framework of CP has not been sufficient to achieve effective participation within the health sector (see Figure 4).
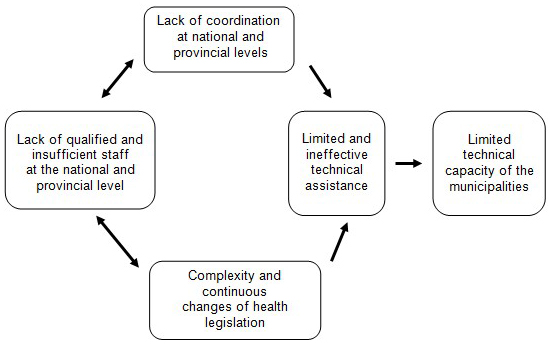
Figure 4: Poor role of the national and provincial health authorities [36]
These codes from interviews are examples of what happened:
"There is no civil organization of the society. That is to say, we are people living together in a geographical area, but we are not organized in a civil society" (EI-1).
"The Communal Action Boards are indistinguishable from the political directorates. This is a very, very political municipality" (EII-2).
"But people have not been able to be involved effectively in health issues, for instance, in controlling the allocation of subsidies for health services. Also, some preventive programs that used to be delivered in the villages were closed and the community has not been able to get them again" (EIB-3). [37]
The previous categories presented problems such as political issues and the lack of technical capacity and autonomy of the municipalities; tensions in the provision of services; the poor role of national and provincial health authorities, and the underdevelopment of community participation, all of which are interrelated. The decentralization process in Colombia has been taking place in a political, economic and social context characterized by armed conflicts between the Army, guerrillas and paramilitary groups, fiscal constraints, cultural values and a political system that affect this process; but new studies would be necessary in order to analyze how this context affects the decentralization process (see Figure 5).
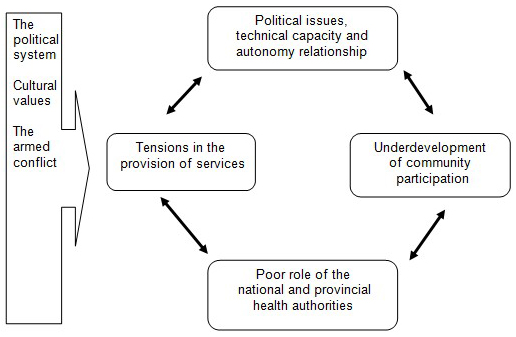
Figure 5: Political and administrative aspects related to the health decentralization process [38]
The findings of this study, in terms of ID and CP, suggest that an integration of the administrative capacity of the majority of municipalities is still insufficient, and that the limited effectiveness of municipal health bodies may be related to their limited technical capacity for making decisions in key functions, due to low professional training of mayors and their staff, which in turn is related to the patronage system. The central government defines many features that must be put in place by the municipalities and regions. This is in contradiction to the concept of decentralization in the form of devolution used in Colombia, which entails more autonomy for municipal governments. [39]
Before decentralization, the health sector was less affected by the patronage system at the municipal level. However, with decentralization, mayors appoint their staff and the director of the public hospital, a situation highly affected by the political patronage and by frequent changes of rulers in the municipalities. These situations have limited the capacity, credibility, trust, leadership and negotiation abilities of the municipal authorities. The private HPEs and ASSs, supported by the Neo-liberal economic context, have taken advantage of the weaknesses of the public sector and of the community in order to achieve their particular interests. Previous studies in Colombia and other Latin American countries showed a very little administrative capacity of municipalities to manage the health sector (BANKAUSKAITE & SALTMAN, 2007; HARTMANN, 1999; MASCAREÑO, 1996; RONDINELLI, 1990). Some studies highlighted the lack of qualified staff as an important limitation to achieve institutional capacity of the health sector and/or of the municipal government (COLLINS, OMAR &TARIN, 2002; NIGENDA & MACHADO, 2000; YEPES & SÁNCHEZ, 2002). However, no previous study had documented the close and pervasive relationship between the staff and the political patronage system, which may be understood within the relationship between the political parties, the political system and the state (ANGELL et al., 2001; ARRUBLA, 1991; NIETO, 1997; ZAMBRANO, 1989). The public institutions are subordinated to the relationship between the state and the political parties; at the same time, they are a means for rulers to either "retain power" or "remain in power" power. Mayors are part of the political chain, which may affect the ability of municipal governments and their health authorities to forge links among different stakeholders, and to mobilize political, economic, social and technical resources in order to foster co-operation and to achieve the goals of the health sector decentralization. The problems identified in relation to the staff have had transcendent implications in several dimensions of ID, CP and in the effectiveness of technical assistance programs. Trained staff members are dismissed and new ones are appointed several times a year. In addition, in many municipalities, when the municipal administration or the rulers change, the outgoing staff removes files, a situation that limits technical capacity and "institutional memory." Thus, the decentralization process is very prone to being affected by the frequent political changes in municipal governments (WILLIS, GARMAN & HAGGARD, 1999). [40]
The findings also revealed a limited development of the health sector surveillance and monitoring system, which is consistent with the outcomes of two previous studies carried out by SILVA et al. (2002) and the National Planning Office (VÉLEZ, 2003). This aspect may be understood within the context of the Neo-liberal economic model, which privileges the private sector and diminishes the role of the state (NORTH & BRADSHAW, 1997). Thus, the limited development of the surveillance and monitoring system may be an "implicit strategy" to allow free growth of the private sector, even at the expense of public resources. Thereby, private HPEs and SSAs become very powerful politically and economically (PELÁEZ, 2005), which has created conflicts and an unbalanced distribution of power among stakeholders. According to AHUMADA (1998), the most important economic elite of the country are the owners of private HPEs and SSAs, who have enough economic, social and political resources to influence decision-making at the highest levels of government. Therefore, it has been difficult for municipal authorities, without enough administrative capacity, to control the private sector without strong timely support from the regional and national bodies. The findings also suggest that there is a growing percentage of the population affiliated to the SSSH; as CÉSPEDES et al. (2000) also showed, the affiliation of the poorest to the SSSH increased from 3.1% in 1995 to 43.7% in 1999 throughout the country. However, the findings also suggest that there have been tensions in the accessibility and quality of services, as well as several market failures, mainly on the part of the private HPEs and ASSs, which were also found in previous studies (ARBELÁEZ et al., 2004; AYALA & KROEGER, 2002). Their profitable interests have created new limitations to access services; these limitations include: cream-skimming, deny of services, geographical barriers—even within the biggest cites—, failures in the contracting process, and reduction in the provision of preventive programs (CHÁVEZ, SIERRA, LOPERA & MONTOYA, 2004). Therefore, to be affiliated to the SSSH is not always a guarantee to gain effective access to services. These conflicts are consistent with those aspects described by BATLEY (1996) and SCOTT (2001) as the sources and expressions of market failure. Also, COLLINS and GREEN (1993) pointed out the risks of mixing up decentralization and privatization, since the market failures produced by privatization could be mistakenly perceived as the results of decentralization. [41]
Results from several sources suggest that there is a limited development of CP in health. The position of managers related to the community organizations has been ambiguous. Although municipal health authorities recognize the importance of involving the community within several processes of the health sector, community organizations have not received the necessary technical and political support from municipal administrations and health authorities. A well-informed community might be more demanding of its rights, which may be a threat to a municipal health authority that has been highly influenced by the patronage system and has limited technical capacity. Limited participation by the community was also found in previous studies (MOSQUERA et al., 2001; RAMIRO et al., 2001); this may be understood within the Colombian economic and social development model, which has historically emphasized representative democracy rather than participatory democracy (RESTREPO, 2001; MORENO et al., 1994). [42]
The findings of this study support the idea that the decentralization of the health sector, as a public policy, is a complex and systemic process in which there is a strong interaction between internal administrative issues and the political patronage system, economic and social context (BANKAUSKAITE & SALTMAN, 2007; ROTH, 2006). As a complex phenomenon, decentralization involves a group of successive initiatives, decisions and actions that deal with health problems (ROTH, 2006; VARGAS, 1999). It entails a close interrelationship between the capacity of the health sector itself, the public and private health organizations, the political groups, and other actors at all levels of government, in which the political, social and economic contexts also play important roles. Within this system of interrelations, the level of progress of ID and CP may depend more on the quality of the staff and the political support of the rulers, within a clientelist system, in each municipality than on the socio-economic category of each municipality. The lack of municipal capacity has limited the autonomy and leadership of health authorities, which in turn has prevented an equal distribution of power among the stakeholders at the municipal level. To create an equal distribution of power among several actors is one of the goals of the decentralization process, understood within a participatory democracy and a pluralistic perspective of the state, which takes time to be built (DAHL, 1984; ROTH, 2006). Bearing in mind the systemic character of the decentralization of the health sector, the findings of this study suggest the need for a trade-off among policies, in order to create co-operation among the stakeholders involved in the sector. Also, the findings support the concept that there is no absolute decentralization; in Colombia, there has been a mixture of devolution—as the main form of decentralization—, delegation and privatization (KUTZIN, 1995). In addition, a higher level of economic development in one municipality does not necessarily mean greater progress for ID and CP. The underlying social capital, political relationships and the political will of groups in each municipality may affect the level of support and the progress of decentralization. Also, the complexity of the bigger municipalities requires more complex negotiation and consensus processes commensurate with higher technical and administrative development. Thus, in the middle size municipalities in categories 3, 4 and 5, which represent 49.3% of the municipalities of the country, it may be easier to put the decentralization process in place and generate better outcomes in the health sector, because there is a simpler network of interrelations and therefore simpler implementation processes. [43]
Guide for the semi-structured interview of municipal health directors, mayors and top-managers of health organizations at the municipal level
Name of (the) municipality ________________________________
Name of (the) organization _______________ Respondent’s position? ________
Institutional development
Effectiveness of the main health administrative entities in the municipality
1. What are your overall thoughts about the effectiveness of the existing management entities (bodies, institutions or organizations) in your municipality?
2. How would you rate the effectiveness of the following municipal health entities in carrying out their functions : (5: Very effective; 4: Effective; 3: Moderate; 2: Not very effective; 1: Ineffective; 0: Inexistent/Not applicable):
___ Municipal Health Department
___ Municipal Health Fund
___ Municipal Council of Social Security for Health
___ Administrators of the Subsidy Scheme
___ Health insurance companies
3. Could you describe the most important obstacles in the operation of the management bodies of health in your municipality?
Human resources
4. Who is in charge of the Municipal Health Department's functions?
5. Could you list the number and qualifications of the staff of the MHD?
6. In your opinion, what are the technical skills and values that the staff involved in health management must have in order to support the decentralization of the health sector at the municipal level?
7. In practice, how important are the following aspects when appointing staff in your health organization? Could you rate the level of importance (05: Very important; 04: Important; 03: Neutral; 02: Unimportant; 01: Very unimportant). Could you explain your answer?
___ Affiliation to a specific political party
___ Experience on health management
___ Professional degree and resume or curriculum vitae
___ Relationship with the mayor
___ Relationship with the municipal council
___ Pressure by the political parties
___ Personal skills for team work
___ Community work experience
8. What kind of professional background and experience in health management do you have?
9. Please rate the extent to which you feel you possess the following qualities: (05: Very high; 04:High; 03: Normal; 02: Low; 01: Very low)
___ Managerial skills in health management
___ Teamwork skills
___ The degree of consistency between your professional background and the functions of your position
___ Professional capacity for providing technical support to the implementation of the health decentralization process
Health planning process
10. What types of health plans did the municipality carry out in 2000? Could you rate the extent to which these plans were carried out?
11. Who participates in the health planning process in this municipality?
12. Could you describe the most serious difficulties encountered in the planning process?
Information system
13. Could you describe the type of data that the Health Information System of this municipality generates today?
14. Could you rate the quality (5: Very good; 4: Good; 3: Moderate; 2: Poor; 1: Very poor) of health information in terms of its reliability, timeliness, comprehensiveness, accuracy and availability?
15. How do you feel about the level of effectiveness (5: Very effective; 4: Effective; 3: Moderately effective; 2: Ineffective; 1: Very ineffective) of health information in making decisions in your municipality?
Supply of services
16. How do you feel about the supply of primary health care in your municipality?
17. What are the most important difficulties in supply services?
Health social security system
18. Number of population covered by the SISBEN and affiliated to the SSSH (from secondary source) __________
19. In your view, what are the most important achievements with regard to the implementation of the Social Security System in Health in your municipality?
20. In your view, what are the main obstacles preventing the implementation of the Social Security System in your municipality?
Processes of quality guarantee of the services
21. Could you list the administrative processes which have been implemented in your institution to ensure a good quality of services? (For instance, accreditation, evaluation of clinical records process, surveys on user satisfaction, surveillance of intra-hospital infection, internal monitoring system, users’ complaints, financial audit and referring patients process, which means the administrative arrangements defined to send a patient from one institution to another in order to provide more complex medical services when the patient needs them).
22. Could you rate their effectiveness in improving the quality of services? (5: Very effective; 4: Effective; 3: Moderate; 2: Ineffective; 1: Very ineffective; 09: Inexistent). Could you explain your answer?
Surveillance and control of the health sector
23. How do you feel quality of the surveillance and control system of the health sector works in your municipality?
24. Could you rate the effectiveness of the following organizations in carrying out monitoring and control functions in your municipality? (5: Very effective; 4: Effective; 3: Moderate; 2: Ineffective; 1: Very ineffective; 09: Inexistent). Could you explain your answer?
___ National Superintendent of Health
___ Public Prosecutor
___ Ombudsman
___ Citizens' watchdog
___ User Associations
Community participation
25. Could you list the community organizations belonging to this municipality?
26. Could you rate the level of effectiveness these organizations have had in decision-making on health issues? (05: Very effective; 04: Effective; 03: Neutral; 02: Ineffective; 01: Very ineffective).
27. Could you describe the main obstacles faced by community organizations in participating in health issues in your municipality?
Additional aspects that have affected decentralization
28. Could you describe the obstacles in the implementation of decentralization in this municipality?
29. Additional comments
1) Law 10 of 1990, Law 60 of 1993 and Law 75 of 2001 constitute the core legislation of the Colombian decentralization process. <back>
2) A Nation is a collection of people of a country who share a similar language and culture; common traditions and have the same government (ZAMBRANO, 1989, p.31). <back>
3) According to BURDEN, COOPER and PETRIE (2000, p.20), "Keynes' theories involved a system of government intervention to increase spending in order to create jobs, whilst preserving the market and individual economic and political freedom." The economic crisis was caused by the lack of demand for goods and services, which needed to be boosted in order to reactivate the economic system (KEYNES, 1968). The State as political actor had the capacity to remove these obstacles and generate other stages of capitalism's accumulation and reproduction through a policy of public investment (NORTH & BRADSHAW, 1997, p.13). However, this model was also a result of conflicts and pressures from social and political groups, which demanded social security and a major economic redistribution of the goods and services produced by society (DESAI, 2000; BURDEN et al., 2000; NIETO, 1997, p.56). <back>
4) NORTH and BRADSHAW (1997) point out that there are four strands or "schools of thought' implicated in Thatcherite neo-liberalism or New Right, and in each one the role of the market is crucial: a) the Austrian minimal state intervention and a free market was the situation most likely to create and encourage freedom through choice; government power should be limited so that the market may respond freely to consumer choice. The components of the market should stand or fall economically on their ability to satisfy the consumer (HAYEK, 1960). b) The Chicago: "monetarism" argued by FRIEDMAN indicates that the fiscal prudence of providers of good and services should actually shape the market; the State should play a more residual role (FRIEDMAN, 1962). c) The Public Choice: the theorists of this strand noted that the interests of those running state services were best served by having a large public sector; this they argued was inherently inefficient as it challenged the hegemony of the market. Where complete removal of the public sector was impossible, they argued for the introduction of pseudo-market discipline and constitutional limitations to the activities of public sector organizations. Public choice perspectives were of growing influence in Britain through the second Thatcher government (NORTH & BRADSHAW, 1997; NISKANEN, 1971). d) The Anarcho-Capitalist: this strand advocates unrestricted freedom, the abolition of the state and a grassroots democratic policy based on individual choice: an atomized market (NOZICK, 1974). <back>
5) The New Right Perspective includes two main strands of thought which have contradicted each other. The first strand is the economic neo-liberal strand, with its ideological commitment to market provision. Market is believed to be, not only the most efficient means of production and distribution of resources, but also the mechanism by which individual freedom will be protected and enhanced. The state can never provide or allocate goods and services as efficiently as the market. It is believed that state provision will restrict individual freedom by limiting individual choice and by imposing taxes to pay for the services provided (JOSEPH & SUMPTION, 1979). The second strand is the Neo-conservative, and advocates a more interventionist role for the State in promoting traditional family values, morality, law and order, citizenship, duty, responsibility and community. A strong State is also thought to be necessary to provide the conditions within which the market can operate efficiently and effectively (NORTH & BRADSHAW, 1997). These two strands of the New Right create conflict, which may express itself when public policies based on those principles are being formulated and implemented. <back>
6) The letters A, B and C are used to name municipalities in order to keep identity and confidentiality of municipalities and their participantsanonymous. <back>
7) SISBEN is a system of population classification according to the socio-economic level. <back>
8) "Not all the Health Promoters Enterprises contract services in the hospitals and health centers of the municipality. Many times patients have to look for services in other municipalities or in the biggest cities" (EIB-2). "The Health Promoters Enterprises make contracts with hospitals from other municipalities to get low prices. They do not contract with the hospitals of this municipality. They do not use the infrastructure that the municipality has, which is not very good" (EILC-4). <back>
9) "The SSAs and HPEs do not pay bills on time to the public hospitals, leading to their financial collapse. They manipulate the negotiation of contracts and pay services to hospitals based on tariffs, which undercut the costs" (EA-2). <back>
10) "The fragmentation and lack of integrity of health services have decreased the quality of services" (EILC-3). <back>
Ahumada, Consuelo (1998). Política social y reforma de salud en Colombia. Papel Político, 7, 1-16.
Angell, Alan; Lowden, Pamela & Thorp, Rosemary (2001). Decentralizing development: The political economy of institutional change in Colombia and Chile. Oxford: Oxford University Press.
Arbeláez, Maria Patricia; Gaviria, Martha; Restrepo, Roman; Franco, Alvaro; Hincapié, Doracelly & Blas, Eric (2004). Tuberculosis control and managed competition in Colombia. International Journal of Health Planning and Management, 19(Suppl.), 25-43.
Arrubla, Mario (1991). Colombia hoy: Perspectivas hacia el siglo XXI (14th ed.). Medellin: Siglo XXI.
Asociación Nacional de Secretarías Municipales de Salud (2000). Base de datos de municipios y departamentos certificados hasta el 2000. Bogotá: Ministerio de Salud.
Ayala, Cerna Carlos & Kroeger, Axel (2002). La reforma del sector salud en Colombia y sus efectos en los programas de control de tuberculosis e inmunización. Cuadernos de Saúde Pública, 18(6), 1.771-1.781.
Ayee, Joseph R.A. (1994). An anatomy of public policy implementation: The case of decentralization policies in Ghana. Aldershot, England: Avebury.
Bankauskaite, Vaida & Saltman, Richard B. (2007). Central issues in the decentralization debate. In Richard B. Saltman, Vaida Bankauskaite & Karsten Vrangbaek (Eds), Decentralization in health care: Strategies and outcomes (pp 9-21), http://www.euro.who.int/document/e89891_overview.pdf [Date of access: May 9, 2009].
Batley, Richard (1996). Public-private relationships and performance in service provision. Urban Studies, 33(4/5), 723-752.
Bennett, Sara; McPake, Barbara & Mills, Anne (1997). Private health providers in developing countries: Serving the public interest? London: Zed Books.
Bloom, Gerald (2001). Equity in health in unequal societies: Meeting health needs in contexts of social change. Health Policy, 57(3), 205-224.
Bourque, Linda & Fielder, Eve P. (1995). How to conduct self-administered and mail surveys. London: Sage.
Bryman, Alan (1988). Quantity and quality in social research. London: Unwin Hyman.
Burden, Tom; Cooper, Charlie & Petrie, Steph (2000). Modernizing social policy: Unrevealing new labor's welfare reforms. Aldershot: Ashgate Publishing Limited.
Burki, Shahid Javed; Perry, Guillermo E. & Dillinger, William (1999). Más allá del centro: La descentralización del Estado. Washington, D.C.: Banco Mundial.
Cardona, Álvaro; Arbeláez, Maria Patricia & Chávez, Blanca (1999). Impacto de la reforma de seguridad social sobre la organización institucional y la prestación de servicios de salud en Colombia. Universidad de Antioquia. Revista Facultad Nacional de Salud Pública, 16(1), 20-40.
Castaño, Ramón A.; Arbeláez, José; Giedion, Ursula & Morales, Luis (2001). Evolución de la equidad en el sistema de salud colombiano. Santiago de Chile: CEPAL-ECLAC.
Céspedes, Juan E.; Jaramillo, Iván; Martínez, Rafael; Olaya, Sonia; Reynales, Jairo; Uribe, Camilo et al. (2000). Reforma de la Seguridad Social en Salud en Colombia y efectos sobre la equidad en el acceso y la utilización de servicios de salud. Revista Salud Pública, 2(2), 145-164.
Chávez, Blanca; Sierra, Oscar; Lopera, Mónica & Montoya, Paula (2004). El Plan de Atención Básica en los municipios descentralizados de Colombia, 2001-2003. Revista Facultad Nacional de Salud Pública, 22(2), 77-99.
Collins, Charles D. & Green, Andrew (1993). Decentralisation and primary health care in developing countries: Ten key questions. Journal of Management in Medicine, 7(2), 58-68.
Collins, Charles D.; Araujo, Jose & Barbosa, Jarbas (2000). Decentralising the health sector: Issues in Brazil. Health Policy, 52(2), 113-127.
Collins, Charles D.; Green, Andrew & Hunter, David (1999). Health sector reform and the interpretation of policy context. Health Policy, 47(1), 69-83.
Collins, Charles D.; Omar, Mayeh & Tarin, Ehsanullah (2002). Decentralization, health care and policy process in the Punjab, Pakistan in the 1990s. International Journal of Health Planning and Management, 17(2), 123-146.
Creswell, John W. & Plano Clark, Vicki L. (2006). Designing and conducting mixed methods research. Thousand Oaks, CA: Sage.
Dahl, Robert (1984). Modern political analysis (4th ed.). Englewood Cliffs, N.J.: Prentice Hall.
Departamento Nacional de Planeación; Misión Social & United Nations Development Programme (1999). Informe de desarrollo humano para Colombia. Bogotá: TM Editores.
Desai, Meghnad J. (2000). Well being or welfare? In Neil Fraser & John Hill (Eds.), Public policy for the 21st century: Social and economic essays in memory of Henry Neuberger (pp.77-93). Bristol: The Policy Press.
Dreachslin, Janice L. (1998). Conducting effective focus groups in the context of diversity: Theoretical underpinnings and practical implications. Qualitative Health Research, 8(6), 813-820.
Dye, Thomas R. (1972). Understanding public policy. Englewood Cliffs, N.J.: Prentice-Hall.
Exworthy, Mark & Halford, Susan (2002). Professionals and the new managerialism in the public sector. Buckingham: Open University Press.
Fernández, Sara & Pastor, María del Pilar (2001). Proyecto municipios centinela: evaluación del Sistema General de Seguridad Social en Salud, Colombia, 1995-1998. Revista Facultad Nacional deSalud Pública, 19, 9-23.
Flick, Uwe (1998). An introduction to qualitative research. London: Sage.
Forero, Clemente; Hidalgo, Carolina & Jimenez, Guisella (1997). Descentralización y participación Ciudadana. Bogotá: TM Editores-CID Universidad Nacional.
Friedman, Milton (1962). Capitalism and freedom. Chicago: University of Chicago Press.
Glaser, Barney G. & Strauss, Anselm L. (1967). The discovery of grounded theory: Strategies for qualitative research. Hawthorne, N.Y.: Aldine de Gruyter.
Greene, Jennifer & Caracelli, Valerie (2003). Making paradigmatic sense of mixed methods practice. In Abbas Tashakkori & Charles Teddlie (Eds.), Handbook of mixed methods in social and behavioural research (pp. 91-134). Thousand Oaks: Sage.
Hartmann, Luis (1999). Decentralizing health: The experiences and policy lessons in Bolivia. Mimeo. Washington: The World Bank
Hayek, Friedrich A. von (1960). The constitution of liberty. London: Routlege and Kegan Paul.
Hill, Michael J. (Ed.) (1997). The policy process: A reader (2nd ed.). London: Prentice Hall/Harvester Wheatsheaf.
Hogwood, Brian & Gunn, Lewis (1997). Why "perfect implementation" is unattainable. In Michael Hill (Ed.), The policy process. A reader (2nd ed.,.pp.217-225). London: Prentice Hall/Harvester, Wheatsheaf
Islam, Anwar & Tahir, Zaffar (2002). Health sector reform in South Asia: New challenges and constrains. Health Policy, 60, 151-169.
Joseph, Keith & Sumption, Jonathan (1979). Equality. London: J. Murray.
Keppel, Geoffrey & Zedeck, Sheldon (1989). Data analysis for research designs: Analysis of variance and multiple regression/correlation approaches. New York: W.H. Freeman.
Keynes, John Maynard (1968). Crítica de la economía clásica. Barcelona: Ariel.
Kutzin, Joseph (1995). Experience with organizational and financing reform of the health sector. Division of strengthening of health services. Geneva: World Health Organization.
La Forgia, Gerard & Homedes, Nuria (1992). Decentralizing health services in Colombia. A review of progress and problems. A report to the World Bank. Washington: The World Bank.
Legemaate, Johan (2002). Integrating health law and health policy: A European perspective. Health Policy, 60, 101-110.
López Murphy, Ricardo (1995). Fiscal decentralization in Latin America. Washington: Inter-American Development Bank.
Mascareño, Carlos (1996). Municipalización de los servicios sociales en América Latina. Caracas: CLAD.
May, Tim (1997). Social research: Issues, methods and process (2nd ed.). Philadelphia: Open University Press.
Miles, Matthew B. & Huberman, A. Michael (1994). Qualitative data analysis: An expanded sourcebook (2nd ed.). Thousand Oaks: Sage.
Montiel, Lenni (1998). Institutional development of local government in a developing country. The case of Venezuela. Ph.D. Thesis, University of Birmingham, Birmingham.
Moreno, Carlos; Herrera, Wilson; De Mattos, Carlos; Restrepo, Darío; Vargas, Alejo & Morales, David (1994). Laberintos de la descentralización. Bogotá: Escuela Superior de Administración Pública
Morse, Janice M. (Ed.) (1994). Critical issues in qualitative research methods. Thousand Oaks: Sage.
Mosquera, Mario; Zapata, Yolanda; Lee, Kelley; Arango, Carlos & Varela, Alejandro (2001). Strengthen user participation through health sector reform in Colombia: A study of institutional change and social representation. Health Policy and Planning, 16(Suppl. 2), 52-60.
Mullen, Penelope & Spurgeon, Peter (2000). Priority setting and the public. Oxfordshire: Radcliffe Medical Press Ltd.
Muller, Frits (1991). Pobreza, participación y salud: casos latinoamericanos. Medellín, Colombia: Editorial Universidad de Antioquia.
Nieto, Jaime R. (1997). Desarrollo y salud: la experiencia contemporánea en Colombia y América Latina. Utopía siglo XXI, 1(1), 51-61.
Nigenda, Gustavo & Machado, María H. (2000). From State to market: The Nicaraguan labour market for health personnel. Health Policy and Planning, 15(3), 312-318.
Niskanen, William A., Jr. (1971). Bureaucracy and representative government. Chicago: Aldine.
North, Nancy & Bradshaw, Yvonne (1997). Perspectives in health care. Basingstoke: MacMillan.
Nozick, Robert (1974). Anarchy, state and utopia. Oxford: Basic Books.
Oppenheim, Abraham N. (1992). Questionnaire design, interviewing and attitude measurement. London: Pinter Publishers.
Patton, Michael Q. (1997). Utilization-focused evaluation: The new century text (3rd ed.). Thousand Oaks: Sage.
Peláez, Jaime Alberto (2005). Durante el 2004, EPS y aseguradoras, fuerte ascenso entre las 100 empresas más grandes de Colombia. Periódico el Pulso, 82, http://www.periodicoelpulso.com.co/html/jul05/observa/monitoreo.htm [Date of access: November 25, 2006].
Penagos, Gustavo (1994). Descentralización administrativa (3rd ed.). Santafé de Bogotá: Librería del profesional.
Plaza, Beatriz; Barona, Ana B. & Hearst, Norman (2001). Managed competition for the poor or poorly managed competition? Lessons from the Colombian health reform experience. Health Policy and Planning, 16(Suppl. 2), 44-51.
Powell, Marcus (1999). An analysis of policy implementation in the Third World. Aldershot: Ashgate Publishing.
Pressman, Jeffrey L. & Wildavsky, Aaron B. (1984). Implementation: How great expectations in Washington are dashed in Oakland (3rd ed.). Berkeley: University of California Press.
Punch, Keith (1998). Introduction to social research. Quantitative and qualitative approaches. London: Sage.
Ramiro, Laurie; Castillo, Fatima; Tan-Torres, Tessa; Torres, Cristina; Tayan, Josefina; Talampas, Rolando et al. (2001). Community participation in local health boards in a decentralized setting: Cases from the Philippines. Health Policy and Planning, 16(Suppl.2), 61-69.
Restrepo, Dario (2001). Participación social: relaciones Estado-sociedad civil. Revista de Salud Publica, 3(3), 20-35.
Rondinelli, Dennis Aron (1990). Decentralizing urban development programs: A framework for analyzing policy. Washington, D.C.: USAID, Office of Housing and Urban Programs.
Roth, Andre Noël (2006). Políticas públicas: formulación, implementación y evaluación. Bogotá: Ediciones Aurora.
Scott, Claudia (2001). Public and private roles in health care systems. Reform experience in seven OECD countries. Buckingham: Open University Press.
Sen, Amartya (2000). Desarrollo y libertad. Barcelona: Planeta.
Silva, Liliana; Herrera, Vicente & Agudelo, Carlos (2002). Promoción, prevención, municipalización y aseguramiento en salud en siete municipios colombianos. Revista de Salud Publica, 4(1), 1-20.
Silverman, David (2000). Doing qualitative research. A practical handbook. London: Sage.
Stake, Robert E. (1994). Case studies. In Norman K. Denzin & Yvonna S. Lincoln (Eds.), Handbook of qualitative research (pp.236-247). Thousand Oaks: Sage
Strauss, Anselm L. & Corbin, Juliet M. (1990). Basics of qualitative research: Grounded theory procedures and techniques. Newbury Park: Sage.
Sunkel, Osvaldo (2006). Auge, crisis y renovación del Estado. Una perspectiva a largo plazo. Revista Foro, 59-60, 187-199.
Superintendencia Nacional de Salud (1995). El recurso humano de la salud en Colombia. Bogotá: Supersalud.
The World Bank (1993). World development report 1993: Investing in health. New York: Oxford University Press.
The World Bank (1995). Local government capacity in Colombia. Beyond technical assistance. Washington: World Bank.
The World Bank (2001). World Bank Annual Report 2001, 1, http://www-wds.worldbank.org/external/default/WDSContentServer/WDSP/IB/2003/01/07/000094946_02122004122025/Rendered/PDF/multi0page.pdf [Date of access: November 25, 2004].
Vargas, Alejo (1999). El estado y las políticas públicas. Bogotá: Almudena Editores.
Vega, Román (2001). Evaluación de políticas de salud en relación con justicia social. Revista de Salud Pública, 3(2), 97-126.
Velásquez, Fabio (1996). Ciudad y participación. Cali: Universidad del Valle.
Vélez, Isolda M. (2003, 11 de enero). Detectan 3 millones de "colados" en el SISBEN. El Colombiano, 7A.
Villa, Fabio (1997). Crisis política y partidos políticos en América Latina. Revista Utopía Siglo XXI, 1(1), 15-25.
Walt, Gill (1994). Health policy: An introduction to process and power. New York: Martin's press.
Willis, Eliza; Garman, Christopher & Haggard, Stephan (1999). The politics of decentralization in Latin America. Latin America Research Review, 34(1), 7-56.
Yepes, Francisco & Sánchez, Luz H. (2002). La descentralización de salud en Colombia. Estudio de casos y controles, http://www.idrc.ca/es/ev-68272-201-1-DO_TOPIC.html [Date of access: June 23, 2004].
Yin, Robert (1994). Case study research: design and methods (2nd ed.). Thousand Oaks: Sage.
Zambrano, Fabio (1989). La invención de la Nación. Contradicciones del sistema político colombiano. Revista Análisis, Conflicto Social y Violencia en Colombia. Documentos Ocasionales, 56, 31-38.
Gloria MOLINA is Associate Professor at the National School of Public Health at the University of Antioquia. Dr. MOLINA holds a M.B.A. in Public Services and a PhD in Health Services Management from the University of Birmingham, England; a Degree in Nursing and a Master’s Degree in the Sociology of Education from the University of Antioquia, Colombia. Her research interest include: health system and health policy analysis, mixed research methods, qualitative and quantitative approaches. Her most recent publications focus on the decentralization and reform of the health sector in Colombia.
Contact:
Gloria Molina
Facultad Nacional de Salud Pública
Universidad de Antioquia
Calle 52 No 62 – 59, office 232
Medellín, Colombia
E-mail: molinag@guajiros.udea.edu.co
Molina, Gloria (2009). An Integrity Perspective of the Health Sector Decentralization in Colombia [43 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 10(2), Art. 5, http://nbn-resolving.de/urn:nbn:de:0114-fqs090256.

Creative Commons Attribution 4.0 International License