Volume 11, No. 3, Art. 1 – September 2010
Writing Therapies—An Ethnographic Approach to Transcultural Therapies
Gesine Sturm, Maya Nadig & Marie Rose Moro
Abstract: The paper presents an ethnographic research in the ethnopsychoanalytic tradition about a specific type of therapy, which was developed in France: the transcultural therapy in a "multicultural group setting." The authors detail the construction of their methodological approach, which relies on the French and the Swiss tradition of ethnopsychoanalytic research. This research buttresses the argument that the work on the therapeutic alliance, mediation and the construction of new meanings are central for this type of work. They also describe this setting as a space for profoundly creative encounters and the development of new meanings coming "from the margins" of French society.
Key words: cross-cultural psychology; migration; therapy; ethnopsychoanalysis; ethnography; grounded theory
Table of Contents
1. Introduction
2. Methodological Approach: An Ethnopsychoanalytic Ethnography of the Therapeutic Space
2.1 Two different traditions of ethnopsychoanalysis
2.1.1 The French tradition of ethnopsychoanalysis
2.1.2 The Swiss tradition of ethnopsychoanalysis
2.1.3 Combining elements from the "French" and the "Swiss" traditions
2.2 The field and the documentation of observations
2.2.1 Extract from fieldnotes about the hospital: A walk leading to the transcultural consultation
2.2.2 Contextualizing the observations
2.2.3 Institutional contextualization: The transcultural consultation at the Avicenne Hospital
2.3 In-depth interpretation of the fieldnotes taken during therapies
2.3.1 The different steps of the interpretation process
2.4 Writing therapies: How to construct a text about the research
3. The Therapy Setting in Action: Extracts From a Transcultural Therapy
3.1 The pre-history of the consultation
3.1.2 The beginning of the therapy
3.1.3 Illustrations of the three main categories: Therapeutic alliance, mediation and the co-construction of cultural representations
3.2 Comments on the case study
4. Voices From the Margins: The Transcultural Therapies as a Third Space
In this paper, we would like to present a research on a specific type of therapy developed in France during the last 30 years in the context of mental health care for immigrants: the transcultural family therapy in the "multicultural group setting" (STURM, 2005). This setting aims to facilitate cultural mediation and transcultural communication by having therapists from different cultural backgrounds work together with a patient or family. When working in this setting, therapists direct specific attention to the subjective experience of migration and to the cultural background of their patients. [1]
Even though the use of the multicultural group setting is restricted to a few centers in France, it has been of major importance for the development of French approaches to mental health care for migrants and it may be considered as paradigmatic for the innovations in French ethnopsychoanalysis (see NATHAN, 1986, 1995; MORO, 1994, 1998, 2002, 2003, 2007). Conducting a detailed analysis of the interactions within this setting therefore seemed to be of specific interest. [2]
One of the main objectives of the research we will present here was to determine how therapists and patients construct a dialogue about culture, belongings and cultural representations during therapy. How do therapists conceive the culture of their patients? What techniques do they use in order to open a dialogue about cultural representations and emic conceptions of distress? How do patients react, what kind of representations and perspectives do they bring in? Which aspects of their narratives are taken up by the therapists, and which other ones are ignored? Does the dialogue about cultural representations open new possibilities for the symbolization and communication of subjective experiences? And, if this is the case, what is voiced during this process and what is silenced? [3]
2. Methodological Approach: An Ethnopsychoanalytic Ethnography of the Therapeutic Space
The research was conceived as an ethnopsychoanalytic ethnography of the therapeutic space and relied on methods rooted in several research traditions. First of all, it was inspired by the interpretative anthropology of Clifford GEERTZ (1973), where detailed fieldnotes (thick descriptions) are used to describe, understand and interpret the networks of meaning which are constructed during specific interactions in a given social and cultural context (see also LÜDERS, 2000). It also responded to inspirations from the "Writing Culture" debate, where questions of authorship, reflexivity and representation of the cultural Other were discussed in a critical way (CLIFFORD & MARCUS, 1986; BERG & FUCHS, 1999).1) [4]
In addition, it included aspects of ethnopsychoanalytic research methods coming from the "French" and the "Swiss" traditions: the analysis of unconscious dimensions of the interactions during the therapy, both on an individual "psychodynamic" level and on a collective level. In both cases, the analysis of counter-transference plays a central role. In the first case it was used in order to understand the conflicts a patient was involved in; in the second case it was used in order to get access to silenced aspects of the therapy as a cultural practice. [5]
2.1 Two different traditions of ethnopsychoanalysis2)
Even though the French and the Swiss traditions of ethnopsychoanalysis share basic theoretical and methodological assumptions, some important differences can be found between these two approaches. On the one hand, these differences are linked to the historical development of ethnopsychoanalysis in the French and German speaking countries. On the other hand, they echo the different institutional contexts ethnopsychoanalytic research and thinking were embedded into. [6]
2.1.1 The French tradition of ethnopsychoanalysis
The French tradition of ethnopsychoanalysis developed on the basis of the methodological work of Georges DEVEREUX (1967, 1972, 1980). Most of the research conducted in this context has a strong "clinical" orientation, using an interdisciplinary perspective in order to understand inner-psychic processes and their relatedness to cultural and social factors (see MORO, 1994; MOUCHENIK, 2004; BOUVILLE, ATLANI-DUAULT, HEIDENREICH & MORO, 2005). [7]
In this research tradition, DEVEREUX's notion of complementarism plays a central role. Complementarism may be defined as a strategy of triangulation for interdisciplinary research projects, where different perspectives on research material are combined. According to DEVEREUX, psychoanalysis provides excellent theoretical and methodological tools, which may be used in order to understand human subjectivity. At the same time, this perspective had to be combined with other perspectives on the research material, especially if the material was taken from transcultural research situations. Otherwise, researchers would be trapped in ethnocentric conceptions of the cultural Other (see DEVEREUX, 1967). The use of different perspectives on this type of research material should be obligatory, but according to DEVEREUX the different perspectives should not be introduced simultaneously. [8]
This means that in complementarist research, the data are submitted to several independent rounds of analysis. In each round, the researcher uses the methods and theories that belong to the disciplines he or she is referring to. At the very end of the research process only, the researcher integrates the results of the different rounds of analysis into a global interpretation from an interdisciplinary perspective.3) [9]
At the Department of Psychology of the University of Paris 13, the introduction of DEVEREUX's complementarism in transcultural research was largely meant to deepen the understanding of clinical dynamics (psychopathology or psychological processes) in transcultural situations. Using knowledge from anthropology and from other social sciences would bring new insights into this material (see MANSOURI & STURM, 2008; SKANDRANI, TAÏEB, REZZOUG & MORO, 2010). [10]
A second point of major importance in DEVEREUX' work is the question of counter-transference in transcultural research situations (DEVEREUX, 1967): DEVEREUX insisted that a researcher should use an analysis of his or her own emotional reactions to the material (observations, interviews) in order to avoid defensive reactions towards frightening aspects of the material.4) In Paris, researchers used the reflection about their counter-transference reactions (in the seminar, sometimes in research supervisions) to avoid distorted perceptions of the data they analyzed, but also to get hold of the unconscious aspects of their material. This could for example mean that the research group gave a feedback on the relation between the researcher and his/her interviewees and helped him/her to relate his/her emotional involvement to these roles. Finally, one could say that the objective of the analysis of counter-transference reaction was to deepen the understanding of the psychodynamics observed in their material. Researchers paid specific attention to the cultural dimension of this counter-transference, asking themselves whether their emotional reaction towards the analyzed material was based on cultural differences or collective representations with regards to the cultural Other.5) [11]
2.1.2 The Swiss tradition of ethnopsychoanalysis
The "Swiss tradition"6) in ethnopsychoanalysis has a slightly different focus. The work of Georges DEVEREUX also inspired the Swiss tradition, but the latter more significantly developed on a critical reflection on the relation between the unconscious and society. It was Paul PARIN and his colleagues who first introduced this critical reflection (PARIN, MORGENTHALER & PARIN-MATTHEY,1963, 2006; for an introduction into these approaches, see REICHMAYR, 2003). This conception of the interrelatedness of culture and subjectivity always included the question of power-relations and tensions between different parts of society. Cultural factors were not only conceived as symbol systems which frame human experience, but also as the result of a conflict-laden process where power-relations are consolidated while becoming part of the over-individual unconscious (see for example the work of ERDHEIM, 1982). [12]
This perspective resulted in a particular focus of ethnopsychoanalytic research in the Swiss tradition. Researchers' endeavors to disclose hidden meanings and power-relations in their material aimed to grasp a deeper understanding of cultural practices (see NADIG, 1986, 1991, 2004). The work on counter-transference reactions was central in this type of research, but the focus was different from that of the research in the French tradition. An analysis of counter-transference reactions helped to get hold of collective dimensions in the material—collective images we may find in our imagination about the cultural Other, ways of relating to the other, ways of constructing spaces of protest and inversion of existing power relations. The analysis of the unconscious dimension of the relation between the researcher and his (her) interlocutors served to get access to hidden meanings and to unconscious dimensions of society.7) In this sense, psychoanalysis was not only conceived as a theory which could help to understand psychic functioning, but also, and maybe above all as a method which could open the way to an understanding of the unconscious—both in clinical and research contexts (REICHMAYR, 2003). [13]
At the department of Cultural Studies of the University of Bremen, the methodological approach of ethnopsychoanalytic studies was basically inspired by the work of Maya NADIG (2000a, 2000b, 2004). Most researchers were trained in cultural anthropology (sometimes also in other social sciences) and most researchers used an ethnographic methodology, often including ethnopsychoanalytic methods and perspectives (see METJE, 2005; MANSFELD, 2007). Subjectivity and the relation between the researcher and the observed were considered and analyzed in detail, as this is done in the tradition of reflexive anthropology. Furthermore, the ethnopsychoanalytic approach aimed to understand both conscious and unconscious aspects of cultural practices and discourses, including hidden or silenced dimensions of observed cultural practices. [14]
2.1.3 Combining elements from the "French" and the "Swiss" traditions
Combining these research traditions did not only mean to confront different methods, but also to develop a global research strategy, which integrated both psychological and anthropological questions. The main researcher (GS) basically used two different contexts in order to develop this approach: the PhD seminar at the University of Paris 13 and the ethnopsychoanalytic interpretation group at the University of Bremen. [15]
While discussing parts of the material with her colleagues at Paris 13, she focused on questions about the therapeutic process and the impact the dialogue on culture had on this process: "Does this therapy provoke changes, is the discussion about 'cultural issues' important for the therapy process?" [16]
Following the idea of complementarism, she submitted the notes from the therapy sessions to a double analysis: First, she worked on the material to contextualize the topics brought up by patients (or therapists). Then she worked on the psychodynamics on a more individual level, to get a better understanding of the inner conflicts and family dynamics the team encountered in the consultations. During this process, the reflection on the emotional reactions of the researcher, in a psychoanalytic supervision, but also in the discussions in the PhD seminar, played an important role. They gave access to relevant aspects of the material, for example the importance of non-verbal exchanges during therapy. [17]
The discussions in the ethnopsychoanalytic seminar in Bremen had a different focus. In this context, the group of researchers understood the therapeutic setting as a representation practice, a negotiation about representations of the self and the other, belongings and identity. While discussing her fieldnotes (including those about associations, astonishments and "irritations"8)) in this setting, the main researcher tried to go beyond the self-understanding of the therapists, to find out more hidden aspects of the cultural practice to be analyzed.9) This time, the focus was not on the individual dynamics of a patient or the interactions within a family, but the unconscious dimensions of the therapeutic technique itself. [18]
2.2 The field and the documentation of observations
The field was defined as the "therapeutic space" created during the interactions between the patients and the team of therapists. The main researcher took over the role of an "informed trainee" and attended all therapy sessions, which took place in one of the two transcultural consultations in a group setting, over one year. The total number of the sessions was 42. As the sessions took place every two months on average, the observations in therapy included one to five sessions with the same person or family, giving an impression of the therapy processes during a year. [19]
The patients were informed that the therapy sessions were documented and gave their permission to use this material for research. This material was completed by documents from the patient's files (including verbatim protocols made by trainees), fieldnotes about other observations in and outside the hospital, as well as notes about discussions with therapists. The main researcher also used a "research journal" where she wrote down associations and emotional reactions to the material, but also theoretical ideas and contextual information. It also included fieldnotes about observations she made outside of the therapy sessions as the following extract. [20]
2.2.1 Extract from fieldnotes about the hospital: A walk leading to the transcultural consultation
"Most patients use public transportation to go to their therapy sessions. Usually, they arrive by tram and get off at the 'Hopital Avicenne'10) stop, right in front of the hospital entrance. At my first visit, I was quite surprised standing in front of an impressive portal at the entrance of the hospital, with arches, columns and an inscription in Arabic letters, which make clear allusions to North African architecture. I found out later that its design dated back to the French colonial era. The hospital was designed in the 30s by M. Mantout—the architect of the famous Mosque in the heart of Paris—and his colleague M. Azema—an Architect for the City of Paris. At that time, they were asked to design a building 'integrating elements of Muslim style' (Shakri, 2002). The result was a spacious complex of buildings in pavilion style, enclosed by a wall and a portal. Even though the hospital entrance is still imposing, the character of the inside parts of the building has changed, due to a lack of space, money and maintenance: the material shows signs of age, everything seems crowded and several prefabricated buildings have been introduced into the enclosure of the hospital. The transcultural consultations take place in the outpatient clinic, housed in one of these prefabricated buildings, but outside of the wall, at a five-minute walking distance from the entrance of the hospital. If it was not for the small sign which indicates that the building belongs to the hospital, it would be mistaken for a small factory or administrative office. Inside, the building is quite simple and barely decorated: photos and objects from all over the world are the only elements that indicate there might be something like a transcultural consultation." (GS, fieldnote, December 2002) [21]
2.2.2 Contextualizing the observations
During the process of interpretation, the different types of fieldnotes were compared to three other types of documentation in order to relate and contextualize them:
documents about specific contexts and life-worlds patients evoked in therapy;
publications of the defenders of the French ethnopsychoanalytic approaches;
documents about the institutional context of the work, about health care organization and about the history of culture sensitive approaches in France. [22]
In the following, we would like to give an example to illustrate the second and third type of contextualizations. [23]
2.2.3 Institutional contextualization: The transcultural consultation at the Avicenne Hospital
The Avicenne Hospital is situated in Bobigny, a rather underprivileged suburb in the northeast of Paris. On the administrative level, the psychiatric consultation is completely integrated into the general hospital and there are several close cooperations between the psychiatric team and the other services, for instance with the emergency ward, with a multiprofessional team working with drug addicts, or with multiprofessional teams working with traumatized patients. At the same time, the team of the transcultural consultation is only partly integrated into the staff of the hospital as a whole, because several therapists, mostly psychologists, work exclusively on transcultural issues, sometimes with part-time jobs, which do not enable them to integrate completely into the team. All the innovations brought forward by the transcultural team were not necessarily taken over by other services. However, some recent initiatives have gone a step further in the direction of a "transcultural opening" of the whole hospital (as the participation in the WHO initiative "Migrant Friendly Hospital" in 2001, http://www.mfh-eu.net/public/home.htm). [24]
The Avicenne hospital is one of the 46 hospitals of the public health care system of Paris and the surroundings (Assistance Publique des Hôpitaux de Paris, AP-HP). Before its integration into this network, it was conceived as a specialized clinic for patients coming from the former French colonies in North Africa. In 1935, it was inaugurated as a "French Muslim Hospital." At that time, the creation of a hospital dedicated to Muslim patients was justified by the idea that there were specific cultural needs, but it was also based on the fear that the French population of the colonial "hub" might be contaminated with infectious diseases brought in by those who came from the colonies—the "margins" (SHAKRI, 2002). When the Avicenne Hospital was integrated into the public health care system in the 1960s, this "culture-specific" (or rather "Muslim specific") approach carried out in the hospital was abandoned and replaced by a general health care approach applied to the whole population of the district. [25]
From the 1980s on, the issue of culture-specific needs concerning immigrants was raised again at the Avicenne hospital, but in a different context: the mental health care question. Serge LEBOVICI, who was the Head of the Child psychiatry outpatient clinic at the time, stated the need to lead a reflection on cultural diversity and belongings in the mental health care of an increasingly diverse population. He invited Tobie NATHAN, a psychologist and psychoanalyst who had been trained by Georges DEVEREUX, to develop new techniques in order to face the specific needs of families with a migration background. [26]
This cooperation led to the development of the ethnopsychoanalytic approach in France.11) "Cultural difference" became a mental health issue in the first place and it was only much later that the question of cultural-sensitive health care was raised in a more general approach, including the need of cultural-sensitive interventions in somatic health care.12) [27]
As we will see later in the case-study, there were processes of "psychologization" of social suffering13) at work—many patients came with clear signs of psychic decompensation14), but in most cases there was a strong impact of the social situation on their suffering. The demand for mental health care led to a conceptualization of this suffering in psychological (or psychiatric) terms, at least on an institutional level (the social security will ask for a diagnosis in psychiatric terms). In this sense, the consultations in the "multicultural group setting" were undoubtedly part of a highly specialized mental health care system, where social suffering was conceived in psychological terms. But within the therapy sessions, we also found quite different movements: the therapists used the discussion about "cultural issues" in order to re-introduce cultural, social and even sociopolitical contexts. This led to a "re-contextualization" where "psychologization" was partly deconstructed and replaced by other frames. The discourse about "cultural difference" therefore often helped to re-introduce the social dimension of the patients' problems. [28]
Before discussing these sociopolitical contexts and their impact on the therapies we observed, we would first like to give a more detailed presentation of the process of interpretation of the material. [29]
2.3 In-depth interpretation of the fieldnotes taken during therapies
When working on the fieldnotes that documented the therapy sessions, the main researcher (GS) often felt quite lost, alternating between the feeling that everything had already been said—by the experienced therapists and in the writings of French ethnopsychoanalysis—and the idea that it would be impossible to find any common factors in such a diverse material because there would be so many ways of interpreting it. On the one hand, the material was extremely structured by the setting itself, and by the interpretations therapists gave to their own interventions. Sticking to this structure would have meant to run the risk of giving a "thin" and almost trivial interpretation of the therapy sessions. Then, there was also the risk of sticking too much to the interpretations therapists gave to their practice—these interpretations were obviously important, but the objective of the research was to go a step further and to go beyond these interpretations. At the same time, the main researcher was sometimes overwhelmed by the diversity of situations, wondering how she could find a guideline for giving a structure to the process of interpretation. These difficulties and the discussions we had together led to the decision to integrate some aspects of the grounded theory method (GLASER & STRAUSS, 1967; STRAUSS & CORBIN, 1990) into the process of interpretation: the elaboration of codes and categories on the basis of an in-depth analysis of the fieldnotes and the use of theoretical memos and a systematic comparison of different therapy situations and different sequences within a therapy. We also integrated the idea of theoretical sampling, using this technique in a more advanced state of the research in order to choose which situations should be submitted to an in-depth analysis, including supervision and discussions within the ethnopsychoanalytic interpretation group at the University of Bremen. [30]
Looking back, we think that the integration of these aspects of the grounded theory methodology was extremely helpful to the research. Cutting the material into short sections and comparing different situations helped the main researcher to take some distance from her first impressions, her emotional involvement and her identifications, but also from the interpretations the therapists gave to their work. [31]
The use of theoretical memos and the acceptance of plural theoretical frameworks also proved extremely helpful to the research because it helped to get hold of the interrelation between the dynamics of a therapy session and the way patients and therapists dealt with the questions of culture and representation. When confronting these memos to the fieldnotes from the therapy sessions, the main researcher was able to explore the dynamics of the therapy process while keeping an eye on the therapy as a cultural practice, which had to be understood within the larger contexts it is embedded into. [32]
2.3.1 The different steps of the interpretation process
In the beginning, the material consisted of fieldnotes, extracts from the patients' files and a "research journal" encompassing an unsorted mix of theoretical ideas, notes about conversations with research colleagues and notes about the main researcher's emotional involvement into the situation—how she felt in the therapy group or how she reacted to a specific clinical situation. [33]
While analyzing this material, GS started to conceptualize "meaningful differences" between different situations. The formulation of these differences was based on a first analysis of the whole material, including notes from the 42 situations observed. It was also based on a first analysis of the notes (or "memos") in the research journal, where observations were linked to theoretical ideas. In the next step, she chose six therapies (with three sessions in average, each of them about two hours long), which should be submitted to a detailed coding process. The choice of these six therapies relied on a theoretical sampling guided by "meaningful differences."15) They could be differences such as "session with or without an interpreter," "sessions with one patient or with a whole family," "successful sessions" and " sessions where therapists have doubts about positive outcomes"; different countries of origin and different types of migration, or different types of problems that led to the consultation. The six therapies were chosen to illustrate several of these "meaningful differences." [34]
This "corpus" which was supposed to be analyzed in the in-depth interpretation was revised and changed when new dimensions appeared during the process of interpretation. The other consultations were not interpreted in the same detailed way, but confronted (in a less formalized way) to the emerging categories. [35]
The six situations that were submitted to the in-depth interpretation were discussed in the research supervision as well as in the multidisciplinary interpretation group in Bremen and/or in the PhD seminar at the faculty of psychology at Paris 13. In the supervision and in the interpretation group in Bremen, we held the discussions on both "raw material" (fieldnotes and extracts of the verbatim protocols) and theoretical ideas. The discussions in the PhD seminar in Paris were not based on an analysis of "raw material," but on short descriptions of the situations. It focused on the understanding of the therapeutic process and the dynamics. [36]
During the coding process, the main researcher developed rather descriptive codes like "therapist evokes his own origins" or "therapist jokes about my German accent while introducing me" while gradually developing more general descriptive and interpretative categories as "opening of the session: salutation." These categories were constantly confronted to the theoretical memos. This gradually led the formulation of more theoretic categories. [37]
Following STRAUSS' procedure (STRAUSS & CORBIN, 1990), three axial categories were elaborated in order to describe and understand central aspects of the therapeutic practice observed: a) the construction of a "therapeutic alliance," b) strategies of mediation, and c) the discussion about different cultural representation systems and emic conceptions of distress. These concepts linked the data to theoretical concepts and were used as axial categories. They will be presented in Section 3.1.3.16) [38]
The implicit and explicit dialogue about culture and belongings could be found in all three axial categories. Indeed, discussions about the patient's belongings and the different social and cultural contexts that were part of their life world often played a crucial role in the construction of a therapeutic alliance. They were also found in processes of mediation: between the family and institutions, between different branches of the family or between spouses. And they were at the center of discussions about the cultural representation systems the patients referred to. [39]
When elaborating the axial categories, we referred to Anselm STRAUSS' coding paradigm.17) But soon we felt the need to adapt this paradigm in order to make it fit with the theoretical background in ethnopsychoanalysis, reflexive anthropology, postcolonial theory and psychoanalytic theory. These theoretical references led to a specific interest into "hidden parts" of the data and a reflection on unconscious dimensions on both individual and collective levels. This is why we decided to include the notion of the unconscious into our version of the coding paradigm: "phenomena" could include lapses or nonverbal expressions; "intervening conditions," "actions" and "interactional strategies" could be based on unconscious reactions on an individual or on a collective level (e.g. defensive reactions).
|
Coding paradigm |
Adaptation for the therapy context |
|
Conditions (phenomena) |
In our research, phenomena may be the specific way a therapist introduces himself, or how he/she formulates an intervention; it may also be the way the patient acts on the non-verbal level. Example (from fieldnotes): Ms D., a young patient from Mali, tries to calm the one-month-old crying baby. It is lying on her lap. She seems to feel uncomfortable in the therapy session and only answers reluctantly to the therapist's questions.: "Ms D. takes the African fabric she was using as a wraparound baby carrier and covers the baby." When asking why, where, how and what happens, we included an interrogation about the relational and unconscious meaning of this gesture (she was not only trying to calm her child, but also trying to calm herself and to show to the therapists that she was feeling uncomfortable). These relational and unconscious dimensions proved to be most important and had therefore to be included into the interpretation process. |
|
Interactions & emotions (Strategies) |
Interactions and emotions included the interpretation of lapses and unconscious or non-verbal dimensions of the interaction. Example: In our example, the therapist's reaction to Ms D.'s non-verbal message helped to talk about her discomfort. "The therapist comments 'That is good, now she doesn't see us any more'." The therapist's comment includes an interpretation of an implicit message (that Ms D. feels uncomfortable because of the size of the group) and also an implicit theory (that the baby feels her mother's discomfort) |
|
Consequences |
The consequences also focus on the relational and emotional outcomes of an interaction. Example: "The baby stops crying. Now Ms K. seems to be far more relaxed." In this case, the inclusion of relational and unconscious dimensions into the coding paradigm permitted to relate the sequence to the theoretical conceptions of a "therapeutic relation" and the construction of a "therapeutic alliance." |
Table 1: Adaptation of CORBIN's and STRAUSS' coding paradigm (2008, p.89) for the analysis of the therapeutic setting [40]
When relating the axial categories and the role "culture" and "cultural representations" played in them, we found that the dialogue about "culture" went far beyond a simple dialogue about the patient's cultural origin. Therapists often referred to their own belongings—real or imaginary—in order to create a relation with the patient, especially in situations where patients expressed the feeling that they could not be understood in the traditional settings provided in French institutions. Sometimes they also enacted cultural difference within the team in order to help the patient to develop new strategies for the integration (or the conscious confrontation) of conflicting norms and positions. Processes of cultural mediation were used in order to contextualize the patients' narratives, but sometimes they were also used in order to open new possibilities of conflict mediation. There were also moments of inversion and contestation of dominant perspectives and power structures, where patients and therapists discussed about the interactions the families had with public services. The discussion about culture did not lead to the reconstruction of fixed cultural frames, but to a re-interpretation of cultural representations. Sometimes this led to a real "patchwork" of new meanings. [41]
2.4 Writing therapies: How to construct a text about the research
As a final step, the construction of a text about the research proved a real challenge for the documentation of the research in the thesis, but also for the design of this article. What kind of text could help the reader to understand the field, the research process and the "groundedness" of our findings? Would it be helpful to illustrate the categories by many examples from different therapies? Or should we give an idea of the different examples by a series of "case-studies"?18) We decided to present a "thick description" (GEERTZ, 1973) of one therapy in this paper, using extracts from fieldnotes and verbatim protocols of the sessions. Even though a single case study is certainly not representative of the multitude of problems the therapeutic team could be confronted with, a deep exploration of the interaction between the patient's problems, the therapeutic process and the way the team was using its therapeutic technique seemed the most appropriate way of exploring how therapists worked. Presenting several sessions of a therapy gives an idea of the therapeutic process and the detailed presentation shows the re-construction and reinterpretation of cultural representations happens at different moments of the therapy. [42]
3. The Therapy Setting in Action: Extracts From a Transcultural Therapy
We will now give a short description of one of the therapies we analyzed during the research. We choose this example because it illustrates the complexity of the dialogue about cultural representations, which includes a process of re-negotiation of cultural and gender identities, a discussion about different life-worlds and a dialogue about family dynamics within a transnational family organization. [43]
We will start the presentation with a short summary presenting the situation, then we will quote and comment some extracts from the data so as to illustrate the main (axial) categories and their interrelatedness. [44]
3.1 The pre-history of the consultation19)
Ms K. is a thirty-five-year-old woman who came to the transcultural consultation at the Avicenne Hospital after having discussed this possibility with her psychologist, who worked in a public center for mother infant care (Centre de Protection Maternelle et Infantile, PMI). She had started to consult with her psychologist four years before, after a miscarriage in late pregnancy. This miscarriage happened only a few days after a dramatic situation where Ms K. had lost her two-year-old daughter in a fire. The psychologist had been working on a more or less regular basis with Ms K., trying to help her to overcome this traumatic loss. In the following years, Ms K. underwent two more miscarriages, losing both unborn children in late pregnancy. According to her psychologist, Ms K. was suffering from traumatic bereavement and the consecutive miscarriages could be understood as a repetition of the traumatic event. The psychologist did not lack knowledge about the treatment of traumatic bereavement, but she had the feeling that she lacked the skills and contextual knowledge which could help to better understand her patient's family situation, the relation to her husband and the larger transnational family context the couple was living in. She felt unable to evaluate and to mobilize the social and symbolic resources her patient had at her disposal. This is why she suggested supplemental therapy sessions to her patient in the transcultural consultation, where these "cultural issues" could be taken up. Ms K. agreed, and she seemed to have important expectations with regard to this supplemental therapy. [45]
3.1.2 The beginning of the therapy
As it is often the case, the therapy team of the transcultural consultation received Ms K. together with the professional who had asked for the therapy, that is to say with the psychologist of the PMI.20) As the relationship between Ms K. and her psychologist was visibly very good, the presence of this professional enabled the team to work in a very intensive way, discussing extremely painful and conflict- laden issues from the very beginning of the therapy. [46]
3.1.2.1 Summary of the first consultation (from fieldnotes)
First of all, Ms K. talked about the loss of her daughter, constructing a detailed narration about the context and the history of her loss, reported here. Right before her daughter's death, Ms K. was living with her husband and her daughter in France. The family did not have much money and Ms K. was still undocumented, as the demand for family reunion was still ongoing. Ms K. had one older daughter staying with her mother in Burkina Faso. Ms K. had migrated five years earlier to follow her husband who had originally come for educational purposes, to continue the studies he had started when living in Saudi Arabia. In France, however, he was not able to carry out this project and he started to work as a taxi driver instead. When their second daughter was born, Ms and Mister K. applied for an accommodation in a public housing, which they could not get due to a lack of accommodations available. Therefore they had to stay in their "apartment," a place Ms K. describes as "some kind of a garage," without heating. In the winter, she would burn coals in the kitchen in order to heat the room. Several days before the death of her daughter, the child had to be admitted to hospital for respiratory problems caused by a high level of carbon acid gas in the apartment. On the day of her death, her parents had left her alone sleeping in the apartment, and when they came back, they found her dead on a burnt out sofa. Ms K. still thinks that this fire was no accident; she remembers that she did not leave any source of fire in the house. She is convinced that her landlord put on the fire, because he was constantly in conflict with the family. But, as she relates in the first session "justice does not want to listen." [47]
A few days later, Ms K. lost the child she was bearing in the sixth month of pregnancy. From then on, she was followed at the mother infant care center. The team of this institution was regularly in contact with Ms K. and they also met her husband on several occasions. The social worker supported the family with the accommodation procedures and they were eventually relocated in a public housing. The family also received support for the ongoing demand for a family reunion, which should grant Ms K. a legal status in France and allow her daughter to come to France. This issue was of particular importance to Ms K. As long as she was undocumented in France, she could not visit her family in Burkina Faso without running the risk of being rejected at the French border when trying to come back. This meant that she could not go see her daughter in Burkina Faso and it also meant that she was cut from the support of her family network. As she explained in the first therapy session in the group, she also had difficulties to handle the fragile relation between her family and her husband's family at a distance. Her husband and his family were practicing Wahhabi Islam, a particularly strict interpretation of Islam21), rejecting all kind of traditional West African thinking and practice. Her own family was practicing what she called "simple Islam," combining more or less openly "traditional" beliefs and practices with Islam.22) As long as Ms K. lived in Burkina Faso, these differences did not lead to particular difficulties. She could always go see her mother to seek her support, including "traditional" assistance that would not require asking. But since she was now living far away and entirely dependent on her husband, she could no longer ask for this kind of assistance without running the risk to offend her husband or his family. Even though she thought she would need specific "traditional" support from her mother, she was afraid to ask for this kind of support for fear that it would lead to a separation from her husband. [48]
3.1.2.2 Comments and aspects of the following sessions
During the three therapy sessions included into the research, the discussion of these issues played a central role. The therapists first tried to show Ms K. that they were able to understand the contradictions and conflicts she was caught up in. Then they used their different cultural backgrounds and contextual knowledge in order to "re-stage" the different positions she was trying to reconcile (see Section 3.1.3.1 to 3.1.3.). They also opened the way to building new meanings in a patchwork mode, where elements of different cultural representations were combined. These representations had to be sufficiently familiar for Ms K. to be meaningful to her, and sufficiently anchored in Islam thought to be acceptable for her husband and his family. [49]
To build a therapeutic alliance with Ms K. within the therapy, therapists applied strategies that were intimately connected to these techniques of mediation and to the work on cultural representations. They bear witness from an extremely creative process where Ms K. constructed new meanings in order to defend her position while giving a voice to some aspects of the subjective experience she was going through (see Section 3.1.3.3). [50]
3.1.3 Illustrations of the three main categories: Therapeutic alliance, mediation and the co-construction of cultural representations
The three main categories were "Working on the therapeutic alliance," "Mediation" and "The co-construction of cultural representations." We will first give a schematic presentation of these three categories and their main subcategories. Then we will use extracts of the case study in order to illustrate how these categories relate to the dynamics within a therapy session.
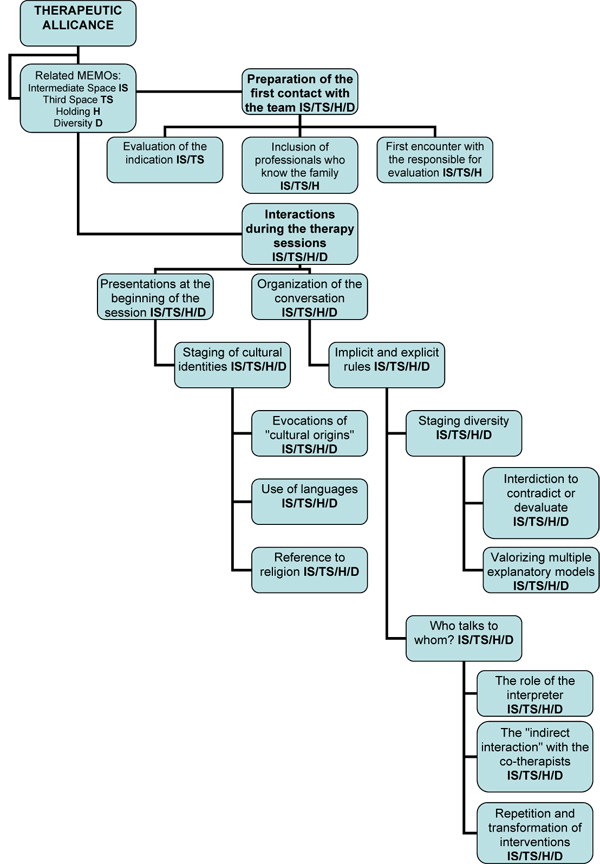
Illustration 1: Therapeutic alliance [51]
In all the sub-categories of this core category, we found two important dimensions which we related later to the theoretical conceptions of an intermediate space (WINNICOTT, 1971) and the third space (BHABHA, 1994). These dimensions concerned the construction of relatedness, proximity and holding and the creation of a space for diversity. [52]
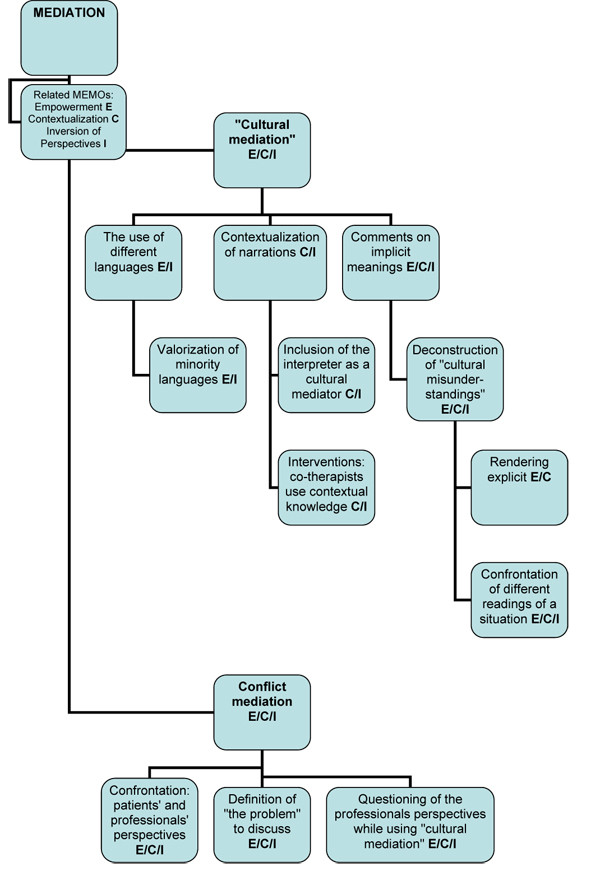
Illustration 2: Mediation [53]
In the sub-categories of this core-category, we found "empowerment," "contextualization," and "inversion of perspectives" as most important dimensions. The conflict mediation and confrontation of perspectives could be put into action once there was a certain alliance with the family. The processes of inversion we found are tightly linked to the work on "cultural mediation." On a conceptual level, we used the conception of the third space in order to discuss this dimension.
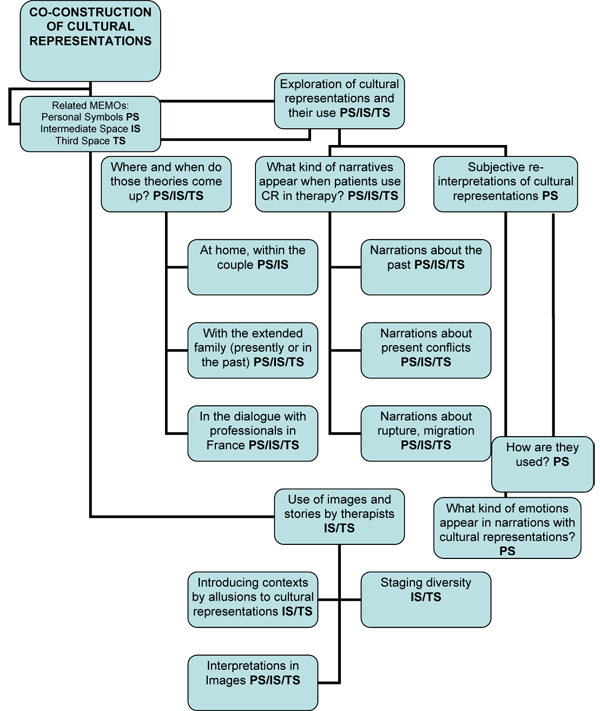
Illustration 3: The co-construction of cultural representations [54]
In the subcategories of this core category, we found out that creativity, the construction of links and bridges between different life-worlds and the creative re-interpretation of existing representations played a central role and became important dimensions of these categories. On a conceptional level, these dimensions are linked to the notion of an intermediate space and the notion of the third space. Very subjective ways of using cultural representations in order to re-interpret current experiences led us to the integration of OBEYESEKERE's concept of personal symbols (1990) into our interpretations. OBEYESEKERE (1990) used this notion to talk about the subjective appropriation of collective symbols. According to OBEYESEKERE, there are two different kinds of processes of symbolization. Symbolizations which are build on the basis of regressive symbols are used to stage inner conflicts without introducing change; symbolizations which are build on the basis of progressive symbols allow for profound changes, for instance a transformation of inner conflicts. OBEYESEKERE'S concepts help to get hold of the dynamics which appear when a person uses collective symbols to reflect on his life. [55]
3.1.3.1 Working on the therapeutic alliance
The term therapeutic alliance designates the collaborative relationship between patient and therapist (GELSO & HAYES, 1998). In the therapy conducted with Ms K., the construction of this alliance was facilitated by the preliminary discussions about her expectations with regard to this therapy, and by the presence of her psychotherapist during the sessions. Ms K. easily accepted the group and relied on the support it offered. Nonetheless, the transcultural consultation team had to "prove" that the therapists within the team were able to understand the conflicts she was involved in. In the first session, therapists brought in contextual knowledge to show Ms K. that they were able to understand her. [56]
The main therapist, a child psychiatrist who was born and trained in Algeria, asked Ms K's psychologist about her patient's origins.
Th[1]23): Where does she come from?
Psy24): Ms K.'s parents are Muslims, Ms K. is Wahhabi and her husband too.
Th[1]: Wahhabi, what is it? Does it have something to do with Islam? (turning to the patient) Wahhabi, it's the kind of Islam you practice?
Ms K.: It's a bit different from normal Islam, but the prayers are the same and Ramadan is the same.
Th[1]: It's the Imam you refer to who is different …
Ms K.: My family practices simple Islam. [57]
At first sight, this session seemed to start on a misunderstanding. While the main therapist asked which country Ms K. comes from, the psychologist introduced her religious affiliation. By doing so, she certainly pointed directly to the most conflict-laden ground, but her formulation also attests that she is unfamiliar with the different forms of Islam. First, the therapist seemed to be following her explanation, then he turned to the patient to give a more precise definition of the difference between Wahhabism and "simple" Islam. During the whole therapy, he introduced contextual knowledge about Muslim religion and culture, taking over the role of "the one who knows Islam." [58]
In the second therapy session, another therapist, who did not attend the first session, introduced himself as being a counterpart. He came from West Africa and one could say that he took over the role of "the one who knows West African cultures." Later, he used this position in order to introduce "traditional" ways of expressing Ms K.'s problems. One particularly interesting sequence occurred when the two therapists used the construction of their respective positions in order to invite Ms K. to build bridges between two types of knowledge: "Islamic knowledge" and "traditional knowledge." [59]
Ms K. had mentioned frightening dreams about a dog biting her, dreams she had experienced each time some days before she lost a child in pregnancy. In the second therapy session, this topic is taken up. The West African therapist asked her about this dream:
Th[2]: Where does the dream happen? In your home country?
Ms K.: No, here. Before I lost F. (her daughter), I had that dream. And only one week later, she was dead. When I get pregnant, I dream of a dog biting me. It is as if somebody was telling me "You will not have this child!" (…)
Th[2]: The dog, what was its color?
Ms K.: Brown or gray or black …
Th[2]: Was it a dog from our place or a dog from here?
Ms K.: Like the dogs at our place, but the color, I do not remember.
Th[2]: Does it bark before biting?
Ms K.: No. [60]
In this section, the therapist constructed closeness by shifting from a discourse where the origins of the patient are represented as "different" ("your home country") to a more intimate relationship where he denoted her origin as a shared position ("our place"). After creating this proximity, he invited the Algerian co-therapists to speak:
Th[2]: Taïeb …?
Th[1]: One has the impression that Ms K. knows that it is a dog, that she can smell the blood running, but she cannot not see. As long as she has not found the reason for F.'s death, it is impossible. In Islam there is a hierarchy and the animal, which is below, is seen as the enemy. This association came to my mind: the enemy is still there and continues to do harm. As long as one is not able to name something, it is impossible to have an image. [61]
In this sequence, the Algerian therapist used references to Muslim imaginary (the idea of the animal as a representation of Sheytane, i.e. the Devil). At the same time, we may note that the underlying logic of his comment is not a religious but a psychodynamic one. Indeed, the therapist used these "religious" images in order to make allusions to the difficulties linked to symbolization in a post-traumatic context. The way he talked about an experience that cannot yet be expressed with words can be seen as a comment on how traumatic experiences cannot be verbalized. It tells us about the work of symbolization in therapy. The verbal expression of the experience is represented instead through the olfactory sense at first. [62]
The West African therapist took up the allusions to Muslim imaginary and invited Ms K. to link them to other, more traditional, representations:
Th[2]: I have a question: Islam proposes this idea of the dog, but in the culture also, what does one say about dogs?
Ms K.: It's the sorcerer.
Th[2]: That is Sheytane?
Ms K.: Yes. [63]
In this sequence, the therapist linked his colleague's comment on symbolization—how to transform sensations into words and images—to an enquiry about the representation systems. In doing so, he tries to help Ms K. symbolize the loss of her daughter. [64]
In the therapy with Ms K., the therapeutic work was organized around a "debate" about the conflicting social and symbolic universes Ms K. had introduced. During the whole therapy, therapists enacted different positions with regard to Islam and to "African traditions" in order to find strategies to reconcile these positions. The therapist from West Africa and the therapist from Algeria, two experienced members of the team, enacted the positions of "the one who knows Islam" and "the one who knows West African Cultures." The other therapists introduced other positions, insisting sometimes on the closeness they had with regard to the patient's position, and using at other times allusions to "distant" locations in order to make propositions without being too direct. [65]
The work on these different positions became a central technique in a work of mediation between Ms K., her husband and his family, but also in the mediation between Ms K. and her psychologist, who came to a deeper understanding of the conflicts her patient was struggling with. To a certain degree, this mediation can be conceived as cultural mediation bridging the gap between different cultural representations and life-worlds (VERREPT, 2008). It also includes an aspect of indirect conflict mediation, where the patient could develop new strategies for negotiating her position within the family. [66]
In the first therapy session, a therapist from Morocco introduced a cultural representation he situated within his own culture: the representation of a child who was born several times, dying each time in early age. By doing this, the therapist located this specific cultural representation in a context, which is simultaneously "close" (African, familiar to the therapist) and "distant" (located in the context of Morocco, far away from the patient's country). He used this device to introduce a cultural representation, which is also very common in West African cultures and well known in Burkina Faso25):
Th[3]: (…) I think about this first fright Ms K. went through, when her daughter was burned. How her fright even frightened the babies she was carrying, how it could rip things out of her womb. She talked about the boys she lost, each time a little bit later, at five, six and seven month of pregnancy. Back home, when there are several consecutive child losses, we say that it is the same boy. (…)
Ms K.: The child that I lost, one may say that, the same person who comes back each time, that is a baby who comes back, back home we say that, too. The old lady cuts a bit from the finger or from the ear. If it is him, he will come back with the same sign.26)
Th[1]: You did not do that?
Ms K.: No, religion does not permit. The first one was incinerated and the second one was incinerated too. Maybe he did not like that? It was my sister-in-law who said that, but as my husband does not like these things … It was the hospital who decided to incinerate them. For the third one, we said no. [67]
In this sequence (as in many other sequences of this therapy), Ms K. went on insisting that she could not refer to "traditional" representations to talk about the loss of her daughter. But this time she did it in a more and more flexible way than before, introducing important aspects of her experience and developing strategies to defend her position. She engaged into a process of exploration and re-interpretation of cultural and religious representations. This happened in a dialogue with the therapists of the team and led to a co-construction of new meanings and cultural representations. [68]
3.1.3.3 The co-construction of cultural representations
Cultural representations are shared symbols that give meaning to human interactions (HALL, 1997). MORO (1998) underlined that these meanings are created in interaction and that the cultural representations evoked within a therapy session must always be understood as the result of a co-construction. Looking at the process of co-construction of cultural representations in our example, we can find interesting processes where different cultural universes are related by a bricolage of meanings. [69]
In the section cited above, Ms K. first recognized that the representation of a child who dies several times could be used in order to describe her problems, provided she was not obligated to refuse it for religious reasons. Then she talked about a "theory" her sister-in-law had developed. Interestingly, this "theory" linked the representation of a child who dies several times to the idea of a transgression with regard to Muslim religious practice. Even though she clearly stated that she could not use this "theory" because her husband would not agree, she used it in order to link her feelings and her way of conceiving the loss of her child with a discourse about religious practice being acceptable for her husband. [70]
Later, she developed a very personal "theory" about her miscarriages, a theory where she introduced a mix of different representations that enabled her to talk about the loss of her daughter. She explained that she kept having dreams of her daughter and that she felt that they "still both needed each other." She stated that "maybe she (her daughter) did not want me to have another child yet." Once she had talked about these dreams, she also explained that she started to feel ready to let her daughter go. At the end of this same session (the second one), she announced that she was pregnant again and asked the group to pray for her. [71]
When she came to the third session some months later, she brought her one-month-old baby with her. She introduced new topics to the session: her position with regard to her husband, her fear that he might repudiate her because the child is a girl and her ideas about the future of her daughter who had just arrived in the household from Burkina Faso. At the same time, she used the therapy session with some consistency. For instance, she relied on the therapists to enact a dialogue where she could consider different ways of living and different cultural representations. Interestingly enough, "French culture" became an important issue in this session, especially when she talked about the future of her children. [72]
3.2 Comments on the case study
If we look at these extracts of Ms K.'s therapy, we can see how much the three central aspects of the therapeutic work are intimately interrelated. While constructing a therapeutic alliance, therapists use techniques of cultural mediation and enactment of cultural diversity, and they also start to discuss, comment and transform cultural representations from the very beginning of the therapy. This happens within a process where the play (in the sense of WINNICOTT, 1971) and the creation of support and holding are very significant. [73]
It is also remarkable that the work on the cultural dimension is completely intertwined with a reconstruction of the actual and past life-world of the patient and that this life-world exists within a sociopolitical and historical context marked by immigration policies and administration processes. The cultural dimension cannot be conceived outside of these fields. Even the most intimate relationships with the family in Africa can only be understood when therapists manage to conceive the inner logics of the family organization and the impact of the migration on the family network. [74]
4. Voices From the Margins: The Transcultural Therapies as a Third Space
On a conceptional level, we used WINNICOTT's notion of an intermediate space (1971) as a heuristic conception, to describe the interactional space that allows the creative processes of constructing new meanings to take place. According to WINNICOTT, the capacity to symbolize and to create cultural representations is based on early experiences of interaction between the child and the caregiver. These early experiences of interaction within an emotionally reassuring relation are fundamental for the creation of the world of shared symbols, which stands between the inner and the outer world. In therapy, the experience of relatedness in a secured environment plays a key-role. It opens the way for the integration of new relational experiences and for the elaboration of traumatic experiences. In our case, we find this process of construction of an intermediate space characterized by the construction of a holding and the opening of a space for creativity on all three levels of the therapeutic work: in the work on a therapeutic alliance, in the processes of mediation and in the work on cultural representation. The construction of this intermediate space is based on emotional reassurance, a holding, but also on therapeutic interventions, which invited the patients to "play" with meanings. [75]
In the therapy we presented in this paper, the construction of a holding was largely supported by the presence of the therapist the patients knew very well, but it was also encouraged by the interventions of the therapists who stressed their familiarity with specific cultural and religious dimensions of Ms K.'s life-world. On the basis of this holding, Ms K. introduced a first narration about the traumatic loss of her daughter. When she talked about this loss later on, she integrated certain aspects of the symbolic worlds that have been mentioned and enacted during therapy, and she did that in a very creative way. This is why WINNICOTT's notion of the intermediate space was very useful to describe these processes in all three key-categories; Yet, another quite relevant aspect came out of the material: processes of inversion. Though this aspect does not really appear in WINNICOTT's work, we considered that this dimension was most relevant in the work with patients coming from minorities. Such moments of inversion of common power-relations played a central role in the therapeutic process (they appear in all three key-categories). For instance, the patient's perspective would be put forward, local languages would be valued, and cultural diversity would be staged within the team of therapists. This led us to use BHABHA's notion of a third space (1994) to describe the relational space created within this type of therapy. According to BHABHA, transcultural encounters at the margins of the dominant society do not only open the door for the exchange of different versions of the world, but they can also bring a new space where new and sometimes quite subversive discourses may be created. [76]
As NADIG (2000a, 2000b) has shown, we may find interesting resemblances between this conception and the concept of an intermediate space in psychoanalytic theory. But BHABHA's notion is of specific interest for the discussion of the transcultural therapies, above all because it explicitly introduces the questions of power, representation and history. These aspects are not often taken up in a direct way in the transcultural consultations. Nonetheless, they are omnipresent, and the discourse about "culture" and "customs" sometimes helps to open the way for a discussion about the relations between "the center" and "the margins"—for instance when discussing the relation between families and institutions, when talking about migration strategies, or about ways of conceiving the cultural Other. [77]
In the therapy with Ms K. processes of inversion can also be identified. They remind us of the "discourse from the margins" described by BHABHA. For instance, when the complexity of West African family relations becomes a central issue within a French institution, or when Ms K. talks about her position as a "fourfold other"27): a migrant, a woman, someone who refers to Muslim religion and culture and someone who equally refers to "traditional" West African knowledge. She develops new positions and ways of contesting dominant ways of conceiving her culture as she starts questioning her different cultural and religious affiliations. Therefore, we may consider that the dialogue with the therapeutic team enhances the process of voicing marginalized positions and we may use the concept of a third space in order to describe these processes. [78]
Yet, we should also consider the limits of these processes of "voicing the marginalized." Some of these limits are linked to the specific role mental health care plays in the context of social and health care for migrants.28) The transcultural therapy sessions are part of a system of mental health care which is tightly entangled with issues of immigration politics (see MBAYE, 2009) and they are also representative of a tendency to use culture-sensitive health care (and especially mental health care) to deal with social and political problems migrants have to face (SARGENT & LARCHANCHE, 2009). This may sometimes have the consequence that the social and political dimensions of the patient's stories may come out of sight, that these stories may become "psychologized." [79]
This clearly shows that the transcultural consultations do not exist outside of the inner contradictions triggered by the separation of mental health care issues from social issues; they are part of a system where social suffering has sometimes to be "psychologized" in order to be heard. Looking at Ms K.'s story, we may for example note that her housing conditions were only improved after the intervention of the psychologist of the multidisciplinary team at the center for mother infant care.29) [80]
At the same time, we may note that the dialogues within the transcultural consultation provoke a movement into the opposite sense of the "psychologization of social problems": a "re-contextualization" where the social, historical and political dimensions of her problems appear, for example when her situation (as undocumented person) with regard to the French administration is discussed. These moments of re-contextualization, where the social dimension of the patients' suffering comes back into the picture, are central to this specific technique of therapeutic work. Cultural representations are not used to replace this social dimension, but rather to enable patients to defend their positions and to voice their subjective experiences. So even though we actually find processes of construction of "cultural difference" at work, these processes open the door to a deconstruction of this same difference: a process where the reflection about difference also helps to create new shared meanings. [81]
1) This means that we did not start from an objectivist conception of the social practice we described, but from a constructivist point of view. We do not conceive the results of our research as an objective representation, but as a—hopefully meaningful and comprehensible—interpretation of the practices we describe. To read about the difference between these conceptions and their impact on qualitative research processes (with a focus on grounded theory research) see MRUCK and MEY (2007). <back>
2) The presentation of these different traditions is largely inspired by the discussions we held at the Summer University "Questions de méthode dans l'ethnopsychanalyse" in 2008 at the University Paris 13 (see http://www.clinique-transculturelle.org/pdf/universite_d_ete_version_longue.pdf). We would like to thank the participants for their inspiring comments! <back>
3) DEVEREUX put forth that each science had specific methods and theories and he urged researchers to avoid blurring the specificity of these instruments by the construction of a mixed interdisciplinary approach. Theories and methods from different sciences should be confronted, but kept strictly separate. In his work, DEVEREUX mainly confronted (ego-) psychoanalytic and anthropologic perspectives. As SALLER (1999) showed in a critical article about DEVEREUX's complementarism, this conception ignores recent developments in cultural anthropology and in psychoanalysis, which make the establishment of clear-cut differences between the focuses of these disciplines more difficult. DEVEREUX did not imagine the development of a reflective turn in cultural anthropology (where subjectivity became central) and the approaches of psychoanalysis he used (mostly ego-psychology) did not focus on the intersubjective aspects of human development. Other approaches brought these aspects into focus (as in object relation theory or in Lacanian theory). This does not necessarily mean that complementarism has been overcome, but it certainly indicates the need to revise this conception, maybe in the sense of a heuristic guideline. <back>
4) Basically, these reactions may lead to a pseudo-objectivist approach to the material where all emotional aspects are ignored. They may also lead to pejorative or exoticizing representations of the cultural Other (see STURM, 2004). <back>
5) MORO (1994) proposes that clinicians and researchers should confront themselves to different cultural frames in order to avoid ethnocentric reactions on material from other cultures. As she formulates it, they should practice their capacity of decentering (décentrage). <back>
6) We refer to a "Swiss" tradition to underline the importance of the work of PARIN and his colleagues ERDHEIM and NADIG in the building of this tradition. Later on, these approaches led to developments in different countries of the German-speaking context (see REICHMAYR, 2003). <back>
7) NADIG's work on the spaces of contestation built by women in rural Otomi culture in Mexico (NADIG, 1986) was fundamental to the development of this type of research. <back>
8) NADIG (1986) proposed to direct specific attention to the "irritations" a researcher may feel when reading his or her research material. The work on these irritations often opens interesting possibilities to understand hidden dynamics in the material. <back>
9) Gesine STURM also submitted extracts of the material to a group of researchers at the Noise European Summer School in Women's Studies "Diasporic Identities and Mediated Cultures: Gender, Power, Representations," held in September 2001 in Madrid. Even though this (feminist) context of discussion did not refer to ethnopsychoanalytic methods or theory, interesting parallels in the interest for hidden power relations were found. <back>
10) The consultation is part of the Avicenne Hospital, a public hospital which is part of the network of the Assitance Publique des Hôpitaux de Paris. For more details, see the analysis in the following. <back>
11) The term "ethnopsychiatry" is also used to denominate the innovations introduced by Tobie NATHAN. This term indicates one important aspect of its creation: the colonial and post-colonial ethnopsychiatry in the former colonies, especially the developments at the hospital of Fann at Dakar, where a social psychiatric model had been combined with a cultural sensitive approach (see COLLIGNON, 2002). <back>
12) SARGENT and LARCHANCHE (2009) showed that this specific development in France led to a certain over-emphasis of the psychiatric dimension of psychosocial suffering in the migrant population. At the same time it also led to very interesting interrogations about the dynamics appearing in transcultural interactions in therapies (STURM, HEIDENREICH & MORO, 2009; STURM, NADIG & MORO, 2010; STURM, BAUBET & MORO, 2010). <back>
13) KLEINMAN's conception of "social suffering" (KLEINMAN, DAS & LOCK, 1997) seems to be helpful in order to underline the fact that the patients did not always conceive their problems in terms of psychic suffering, but rather in terms of social problems and conflicts. <back>
14) Those signs of decompensation could be very different in terms of the diagnostic categories applied to describe their suffering. Diagnostic categories included depression, anxiety disorders, posttraumatic stress reactions, personality disorders and a few cases of psychotic disorders in those cases where an adult person was designated as "the patient." In other cases, where therapies were proposed in response to the suffering of a child, diagnostic categories included disorders linked to learning and development, language acquisition, but also more severe troubles like psychotic disorders or autism. <back>
15) As the methodological approach was rather unusual for the researchers at the department of Psychology at Paris 13, we preferred to define an "acceptable number of cases" for the in-depth analysis. We are aware that this strategy is not conform to the proceedings in grounded theory research projects (see MORSE, 2007). As it was possible to include other cases and redefine the corpus during the research project, the selection of these six cases for the in-depth analysis did not prove to be a major restriction to the research. <back>
16) These axial categories integrated different theoretical conceptions: the concept of therapeutic alliance (for the application of this concept on ethnopsychoanalytic therapies, see LEVY and STURM (2002), the concept of mediation (see VERREPT, 2008) and the concept of personal symbols of OBEYESEKERE (1990). <back>
17) For a discussion on Anselm STRAUSS' coding paradigm and its differences with regard to GLASER's strategies to link the material to theoretical conceptions, see KELLE (2007). <back>
18) As TIMMERMANS and TAVORY showed, the choices with regard to a written representation of the results of an ethnographic research may be quite variable. While classical ethnographies use detailed thick descriptions in order to depict the situational aspect of the research, sociological ethnographies with grounded theory methodologies often use a description (and discussion) of their concepts as a framework for the final text (TIMMERMANS & TAVORY, 2007). <back>
19) This summary relies on fieldnotes and on the patient's files at the hospital. To preserve the confidentiality, we changed the name of the patient as well as some elements of her story. <back>
20) This strategy was originally developed by Tobie NATHAN, who invented the multicultural group setting (1986, 1995). According to NATHAN, the participation of professionals knowing the patients should enhance discussions about the patient in his or her presence. NATHAN conceived this type of discussion as appropriate for patients who were used to consultations in "traditional healing contexts" because the logics of "talking about" instead of "asking questions" would be more familiar to these patients. In our research, we developed a different interpretation of the effects of this technique. Above all, it opened interesting possibilities of mediation between professional logics and the family's conception of their problem. <back>
21) The Wahhabi Islam goes back to the writings of Muhammad Ibn al-Wahhab. The Wahhabi interpretation of Islam is often identified with radical or extremist positions, but it also includes moderate positions (DELONG-BAS, 2007) <back>
22) The parallel or combined use of different healing traditions and the co-existence of Muslim religion with more "traditional" religions and healing practices is quite common in West Africa (FASSIN, 1991; AMSELLE, 1990; POPPER-GIVEON, 2009). <back>
23) Th = Therapist, the numbers are used in order to distinguish the main therapist (Th[1]) from the other co-therapists (Th[2] etc.). <back>
24) Psy = Psychologist <back>
25) The representation of a "child who dies and who is born again" has been broadly described by ethnographers (COLLOMB, 1980). It plays an important role in West African cultures and it may even be found in contemporary African literature, as in the famous novel "The Famished Road" from Ben OKRI (1993). <back>
26) She made allusion to traditional healing practices where the dead child will be marked in order to unveil his "real nature" and to discourage him from coming back. <back>
27) We refer to the concept of the colonized woman as a "twofold other" (PETERSON & RUTHERFORD 1986). <back>
28) MBAYE (2009) shows the intimate entanglement of health and immigration politics in France, which sometimes leads to mobilizing health care resources for social or administrative problems. SARGENT and LARCHANCHÉ (2009) also show the importance of culture-sensitive health care approaches in the confrontation with social and political problems in France. <back>
29) This does not mean we question the psychological dimension of Ms K.'s suffering. Indeed, she had developed important symptoms of psychic distress and the proposition of psychotherapy was certainly appropriate. However, we think that the absence of a social response to her suffering led to the development of a situation causing her psychic suffering. <back>
Amselle, Jean-Loup (1990). Logiques métisses. Anthropologie de l'identité en Afrique et ailleurs. Paris: Payot.
Berg, Eberhard & Fuchs, Martin (1999). Phänomenologie der Differenz. Reflexionsstufen ethnographischer Repräsentation. In Eberhard Berg & Martin Fuchs (Eds.), Kultur, soziale Praxis, Text. Die Krise der ethnographischen Repräsentation (pp.11-108). Frankfurt/M.: Suhrkamp.
Bhabha, Homi (1994). The location of culture. London: Routledge.
Bouville, Jean-François; Atlani-Duault, Laëtitia; Heidenreich, Felicia & Moro, Marie Rose (2005). Se protéger en exil. L'attachement chez les enfants de familles en demande d'asile. L'autre. Cliniques, cultures et sociétés, 6(3), 385-97.
Clifford, James & Marcus, George E. (Eds.) (1986). Writing culture. The poetics and politics of ethnography. Berkeley: University of California Press.
Collignon, Réné (2002). Pour une histoire de la psychiatrie coloniale française: A partir de l'exemple du Sénégal. L'autre. Cliniques, cultures et sociétés, 3(3), 455-480.
Collomb, Henri (1980). L'enfant qui part et qui revient ou la mort du même enfant. In E. James Anthony & Cyrille Koupernik (Eds,), L'enfant dans la famille (pp.354-62). Paris: PUF.
Corbin, Juliet M. & Strauss, Anselm L. (2008). Basics of qualitative research: Techniques and procedures for developing grounded theory. Los Angeles: Sage.
Delong-Bas, Natana J. (2007). Wahhabi Islam: from revival and reform to global jihad. London: Tauris & Co.
Devereux, Georges (1967). From anxiety to method in the behavioural sciences. The Hague: Mouton & Co.
Devereux, Georges (1972). Ethnopsychanalyse complémentariste. Paris: Flammarion.
Devereux, Georges (1980). Basic problems in ethnopsychiatry. Chicago: University of Chicago Press.
Erdheim, Mario (1982). Die gesellschaftliche Produktion von Unbewusstheit. Eine Einführung in den ethnopsychoanalytischen Prozess. Frankfurt/M.: Suhrkamp.
Fassin, Didier (1991). Pouvoir et maladie en Afrique: anthropologie sociale dans la banlieue de Dakar. Paris: PUF.
Geertz, Clifford (1973). The interpretation of cultures. New York: Basic Books.
Gelso, Charles J. & Hayes, Jeffrey A. (1998). The psychotherapy relationship: Theory, research and practice. New York: Wiley.
Glaser, Barney G. & Strauss, Anselm L. (1967). The discovery of grounded theory. Strategies for qualitative research. New York: Aldine de Gruyter.
Hall, Stuart (1997). Representation: Cultural representations and signifying practices. London: Open University Press/Sage.
Kelle, Udo (2007). The development of categories: Different approaches in grounded theory. In Anthony Bryant & Kathy Charmaz (Eds.), The Sage handbook of grounded theory (pp.191-213). Los Angeles: Sage.
Kleinman, Arthur; Das, Veena & Lock, Margaret (Eds.) (1997). Social suffering. Oxford: Oxford University Press.
Lévy, Katherine & Sturm, Gesine (2002). Tissage de l'alliance thérapeutique en consultation transculturelle: quelques fils. Champ Psychosomatique, 25, 57-68.
Lüders, Christian (2000). Beobachtungen im Feld und Ethnographie. In Uwe Flick, Ernst von Kardoff & Ines Steinke (Eds.), Qualitative Forschung (pp.151-153). Reinbek: Rowohlt.
Mansfeld, Christine (2007). Vom Dogonland nach Bamako. Diskurspraxen zu Gender und Migration am Beispiel der Mädchenjugend in Mali. Frankfurt/M.: Brandes & Aspel.
Mansouri, Malika & Sturm, Gesine (2008). Reflet du racisme le voile: emblème d'un métissage conflictuel. L'autre. Cliniques, cultures et sociétés, 9(3), 381-400.
Mbaye, Elhadj Mamadou (2009). Contradictions in public policies: Immigration and the struggle against Aids in France. International Journal on Migration, Health and Social Care, 5(3), 33-39.
Metje, Ute (2005). Zuhause im Übergang. Mädchen und junge Frauen am Hamburger Hauptbahnhof. Frankfurt/M.: Campus.
Moro, Marie Rose (1994). Parents en exil. Paris: PUF.
Moro, Marie Rose (1998). Psychothérapie transculturelle des enfants de migrants. Paris: Dunod.
Moro, Marie Rose (2002). Enfants d'ici venus d'ailleurs. Naître et grandir en France. Paris: La Découverte.
Moro, Marie Rose (2003). Parents and infants in changing cultural context: Immigration, trauma and risk. Infant Mental Health Journal, 24(3), 240-64.
Moro, Marie Rose (2007). Aimer ses enfants ici et ailleurs. Histoires transculturelles. Paris: Odile Jacob.
Morse, Janice M. (2007). Sampling in grounded theory. In Anthony Bryant & Kathy Charmaz (Eds.), The Sage handbook of grounded theory (pp.229-245). Los Angeles: Sage.
Mouchenik, Yoram (2004). L’enfant vulnerable. Psychothérapie transculturelle en pays kanak (Nouvelle-Calédonie). Grenoble: La pensée sauvage.
Mruck, Katja, & Mey, Günter (2007). Grounded theory and reflexivity. Anthony Bryant & Kathy Charmaz (Eds.), The Sage handbook of grounded theory (pp.515-538). Los Angeles: Sage.
Nadig, Maya (1986). Die verborgene Kultur der Frau. Gespräche mit Bäuerinnen in Mexiko. Subjektivität und Gesellschaft im Alltag von Otomi-Frauen. Frankfurt/M.: Fischer.
Nadig, Maya (1991). Formen gelebter Frauenkultur. Ethnopsychoanalytische Fallstudien am Beispiel von drei Frauengenerationen des Züricher Oberlandes. Zürich: Nationalfonds Zürich.
Nadig, Maya (2000a). Interkulturalität im Prozess – Ethnopsychoanalyse als methodischer und theoretischer Übergangsraum. In Hildegard Lahme-Gronostaj & Marianne Leuzinger-Bohleber (Eds.), Identität und Differenz. Zur Psychoanalyse des Geschlechterverhältnisses in der Spätmoderne (pp.87-101). Opladen: Westdeutscher Verlag.
Nadig, Maya (2000b). Zur (Re)konstruktion gemeinsamer Bedeutungen im interkulturellen Begegnungsprozeß. In Judith Schlehe (Ed.), Zwischen den Kulturen zwischen den Geschlechtern. Kulturkontakte und Genderkonstrukte (pp.37-52). Münster: Waxmann.
Nadig, Maya (2004). Transculturality in process. Theoretical and methodological aspects drawn from cultural studies and psychoanalysis. In Hans-Jörg Sandkühler & Lim Hong-Bin (Eds.), Transculturality, epistemology, ethics, and politics (pp.9-21). Frankfurt/M.: Peter Lang.
Nathan, Tobie (1986). La folie des autres. Traité d'ethnopsychiatrie clinique. Paris: Dunod.
Nathan, Tobie (1995). L'influence qui guérit. Paris: Odile Jacob.
Obeyesekere, Gannanath (1990). The work of culture. Symbolic transformation in psychoanalysis and anthropology. Chicago: The University of Chicago Press.
Okri, Ben (1993). The famished road. New York: Anchor Books.
Parin, Paul; Morgenthaler, Fritz & Parin-Matthèy, Goldy (1963). Die Weissen denken zuviel. Psychoanalytische Untersuchungen bei den Dogon in Westafrika. Zürich: Atlantis.
Parin, Paul; Morgenthaler, Fritz & Parin-Matthèy, Goldy (2006). Fürchte deinen Nächsten wie dich selbst. Psychoanalyse und Gesellschaft am Modell der Agni in Westafrika (2nd ed.). Gießen: Psychosozial Verlag.
Peterson, Kirsten Holst & Rutherford, Anna (Eds.) (1986). A double colonization: Colonial and post-colonial women's writing. Aarhus: Dangaroo Press.
Popper-Giveon, Ariela (2009). Adapted traditions: The case of traditional Palestinian women healers in Israel. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 10(2), Art. 11, http://nbn-resolving.de/urn:nbn:de:0114-fqs0902119 [accessed: August 16, 2010].
Reichmayr, Johannes (2003). Ethnopsychoanalyse. Geschichte, Konzepte, Anwendungen. Gießen: Psychosozial Verlag.
Saller, Vera (1999). Die Bedeutung des Kulturbegriffs für psychoanalytische Therapien. In Fernanda Pedrina, Vera Saller, Regula Weiss & Mirna Würgler (Eds.), Kultur, Migration, Psychoanalyse. Therapeutische Konsequenzen theoretischer Konzepte (pp.99-148). Tübingen: edition diskord.
Sargent, Carolyn & Larchanché, Stéphanie (2009). The construction of "cultural difference" and its therapeutic significance in immigrant mental health services in France. Culture Medicine and Psychiatry, 33(2), 2-20.
Shakri, R. (2002). L’histoire coloniale de l’hôpital Avicenne franco-musulman à Bobigny, http://survivreausida.net/a2965-l-histoire-coloniale-de-l-hopital-avicenne-f.html [accessed: August 16, 2010].
Skadrani, Sara; Taïeb, Olivier; Rezzoug, Dalila & Moro, Marie Rose (2010/in press). The rule of virginity and young women of Maghrebine origin in migration. Transcultural Psychiatry.
Strauss, Anselm L. & Corbin, Juliet M. (1990). Basics of qualitative research. Grounded theory procedures and techniques. Newbury Park: Sage.
Sturm, Gesine (2004). Le racisme et l'exclusion. In Marie Rose Moro, Quiterie de la Noë & Yoram Mouchenik (Eds.), Manuel de psychiatrie transculturelle (pp.265-278). Grenoble: La pensée sauvage.
Sturm, Gesine (2005). Les thérapies transculturelles en groupe "multiculturel". Une ethnographie de l'espace thérapeutique. Unpublished doctoral dissertation in Psychology and Cultural Studies. University of Paris XIII (France) and University of Bremen (Germany).
Sturm, Gesine; Baubet, Thierry & Moro, Marie Rose (2010/in press). Culture, trauma and subjectivity: The French ethnopsychoanalytic approach. Traumatology.
Sturm, Gesine; Heidenreich, Felicia & Moro, Marie Rose (2009). Transcultural clinical work with immigrants, asylum seekers and refugees at Avicenne Hospital, France. International Journal on Migration, Health and Social Care, 5(1), 33-40.
Sturm, Gesine; Nadig, Maya & Moro, Marie Rose (2010/in press). Current developments in French ethnopsychoanalysis. Transcultural Psychiatry.
Timmermans, Stefan & Tavory, Iddo (2007). Advancing ethnographic research through grounded theory practice. In Anthony Bryant & Kathy Charmaz (Eds.), The Sage handbook of grounded theory (pp.493-512). Los Angeles: Sage.
Verrept, Hans (2008). Intercultural mediation: An answer to healthcare disparities? In Carmen Valero-Garcés & Anne Martin (Eds.), Crossing borders in community interpreting: Definitions and dilemmas (pp.187-201). Amsterdam: John Benjamin's Translation Library.
Winnicott, Donald W. (1971). Playing and reality. New York: Basic Books.
Gesine STURM is Lecturer at the Department of Psychology at the University of Paris 13 and member of the Institute of Cultural Studies at the University of Bremen (bik) in Germany. Her research and teaching concerns transcultural therapies, cultural broking in the field of social and mental health care, and ethnopsychoanalytic research methods.
Contact:
Gesine Sturm
Université Paris 13, Département de Psychopathologie Clinique de l'Enfant et de la Famille
Centre de recherches en clinique transculturelle
74, rue Marcel Cachin
F-93003 Bobigny Cedex, France
E-mail: gesine.sturm@gmail.com
Maya NADIG is Professor of European Ethnology at the Department of Cultural Studies at the University of Bremen in Germany. Her teaching and research is focused on ethnopsychoanalytic methods and theories, postcolonial cultural theories, migration, transculturality and identities in the context of globalization.
Contact:
Maya Nadig
Universität Bremen
Fachbereich Kulturwissenschaften
Postfach 33 04 40
D-28334 Bremen, Germany
E-mail: mnadig@uni-bremen.de
Marie Rose MORO is Professor of Child and Adolescent Psychiatry at the University of Paris 5. Her teaching and research concerns transcultural psychiatry, psychopathology and intergenerational relations in the context of migration and globalization. She is in charge of the Department of Child and adolescent Psychiatry d'Avicenne and adolescent psychiatry of Cochin Hospital in Paris (France).
Contact:
Marie Rose Moro
Maison des Adolescents Hôpital Cochin
97, bd du Port Royal
F-75014 Paris, France
E-mail: marie-rose.moro@cch.aphp.fr
URL: http://www.clinique-transculturelle.org/
Sturm, Gesine; Nadig, Maya & Moro, Marie Rose (2010). Writing Therapies—An Ethnographic Approach to Transcultural Therapies [81 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 11(3), Art. 1, http://nbn-resolving.de/urn:nbn:de:0114-fqs100319.

Creative Commons Attribution 4.0 International License