Volume 17, No. 2, Art. 22 – May 2016
Embodied Ways of Storying the Self: A Systematic Review of Body-Mapping
Adèle de Jager, Anna Tewson, Bryn Ludlow & Katherine M. Boydell
Abstract: The first recorded instance of whole-body-mapping for research purposes is a comparison of women's identity and the concept of the reproductive system in rural Jamaica and the UK. It was later developed in a structured workshop process in South Africa to give voice to the experiences of HIV positive individuals, decrease stigma, and advocate for provision of anti-retroviral medication. Whole-body mapping involves tracing around a person's body to create a life-sized outline, which is filled in during a creative and reflective process, producing an image representing multiple aspects of their embodied experience. Body-mapping holds promise as a qualitative, participatory research method to produce and disseminate knowledge. However, it is unclear how it is being used, by whom, and in what context. This article presents the findings of a systematic review of body-mapping in the published literature. The review identifies various implementations of body-mapping in research, therapeutic, and educational contexts. The degree of emphasis on social justice, knowledge translation, research, and therapeutic benefit varies a great deal, as does the intent and use of body-mapping. While body-mapping holds promise, more empirical investigation would be valuable in determining its characteristics in research, clinical, educative and political spheres.
Key words: body-mapping; embodiment; narrative; participatory research; knowledge translation; qualitative research; arts-based; visual methods
Table of Contents
1. Introduction
2. Body Mapping Attributes
2.1 Social justice
2.2 Embodied awareness
2.3 Knowledge production and translation
3. Purpose of the Study
4. Methods
4.1 Search strategy
4.2 Data extraction
4.3 Evaluation of adherence to operationalized definition of body-mapping
5. Results
5.1 Descriptive numerical summary
5.2 Thematic analysis
5.2.1 Body-mapping as a means of sharing stories; research co-production
5.2.2 Body-mapping as political advocacy
5.2.3 Body-mapping as communication/installation
5.2.4 Body-mapping as a teaching tool / education
5.2.5 Body-mapping for examining embodied experience in physical space
5.2.6 Body-mapping as child/adolescent centered method
5.2.7 Body-mapping as therapy/healing
5.3 Reflections on the use of body-mapping
5.3.1 Benefits of body-mapping to participants
5.3.2 Appropriateness of body-mapping to examine social relationships / processes
5.3.3 Suggested future uses and lessons learned
6. Discussion
6.1 Benefits and potential pitfalls of body-mapping
6.2 Embodied experience
6.3 Knowledge translation
6.4 Evolution of mapping the self
6.5 Critique of body-mapping as a research method and therapeutic intervention
6.6 Suggestions for future use
6.6.1 Digital body-mapping
6.6.2 Global health perspective
7. Conclusion
Qualitative research methods provide access to research participants' lived experience (TOLES & BARROSO, 2014) and provide richly textured detail of the social contexts in which these lives are lived. They are also amenable to examination of the meaning that participants make of their experience, and in turn, how researchers interpret these understandings (BROGDEN, 2010). In the context of health-care, Australian government policies and funding organizations over recent years have focused on client-centered care and the involvement of consumers in all aspects of service delivery (AUSTRALIAN COMMISSION ON SAFETY AND QUALITY IN HEALTHCARE, 2011; BYRNE, HAPPELL, WELCH & MOXHAM, 2013; KITSON, MARSHALL, BASSETT & ZEITZ, 2013), New Zealand (ROYAL AUSTRALIAN & NEW ZEALAND COLLEGE OF PSYCHIATRISTS, 2014) Canada (CANADIAN INSTITUTE FOR HEALTH INFORMATION, 2012; CANADIAN MEDICAL ASSOCIATION, 2009; VERMA, PETERSON, SAMIS, AKUNOV & GRAHAM, 2014) and the UK and US (GOUGH & DEATRICK, 2015; RING, RITCHIE, MANDAVA & JEPSON, 2011). This approach is encapsulated in the slogan "nothing about me without me" (DAVIS, SCHOENBAUM & AUDET, 2005, p.953). Thus there is a political imperative to better understand consumer and carer perspectives and the conditions within which they receive health care services and support. Qualitative methods are well suited to this objective and it is unsurprising that their use has increased dramatically over the past two decades (GOUGH & DEATRICK, 2015; TOLES & BARROSO, 2014). While most qualitative research has been textually based, more comprehensive epistemologies that embrace different forms of knowledge have highlighted the potential of visual methodologies in the study of health and illness, particularly the ways in which participants interpret, give meaning to, and make sense of their experiences (GUILLEMIN & DREW, 2010; HARRISON, 2002). Visual methods are a powerful tool for eliciting individual experiences and thus offer researchers new dimensions from which to view a phenomenon (BALL & GILLIGAN, 2010; RAPPORT, 2004). Consequently, interest in arts-based health research methods has burgeoned over recent years (BOYDELL, GLADSTONE, VOLPE, ALLEMANG & STASIULIS, 2012a). Correspondingly, there has been increased development and discussion of methods for conducting visual research, approaches to analysis of visual data and consideration of dissemination, context and audience (CHRISTMANN, 2008; KNOBLAUCH, BAER, LAURIER, PETSCHKE & SCHNETTLER, 2008). [1]
The focus of this review concerns body-mapping, a visual, arts-based process. The first recorded use of whole-body maps can be found in MacCORMACK and DRAPER's (1987) work. They sought to investigate the high fertility rate in rural Jamaica compared to the UK in a cross-cultural study. At the time of this study, fertility in Jamaica gave young women immediate adult status in their families (ibid.). With a focus on fertility, the body-mapping process revealed differing levels of awareness of body regions in the torso area between Jamaican women and university students from the UK (ibid.). Jamaican notions of embodiment in this case align more closely with African body awareness than Western notions of embodiment, as Jamaican women participants shared their African familial practice of burying their umbilical cords under a tree (ibid.). Body-mapping including the whole body was subsequently developed (to our knowledge without the influence of MacCORMACK and DRAPER's work) in South Africa. Created as a means of decreasing stigma associated with Human Immunodeficiency Virus / Acquired Immune Deficiency (HIV/AIDS), it was used to raise awareness and protest the lack of affordable and accessible antiretroviral medication (MacGREGOR & MILLS, 2011). Created as part of the Lifelong and Memory Box Projects1) facilitated by clinical psychologist Jonathan MORGAN and researcher Kylie THOMAS, with a facilitator's guide developed by Jane SOLOMON (2002), the body-mapping process was intended to be therapeutic, creating a space to explore issues which were difficult to discuss and witness experiences which were obscured or hidden (MORGAN & BAMBANANI WOMEN'S GROUP, 2003; STEVENS & LE ROUX, 2011; VASQUEZ, 2004). It was also initially intended as a preparation for death, with participants weaving together memories and stories to leave behind as a legacy for their children (NÖSTLINGER, LOOS & VERHOEST, 2015). However, the focus of the workshops shifted in accordance with increased availability of effective medications to the experience of living with HIV/AIDS. The body-mapping process developed by SOLOMON (2002) involved several arts-based, reflective group workshops held over numerous weeks. Participants traced a life-sized image of their body onto a large cloth or piece of paper and used paint or other art materials to decorate their body-map, including symbols that were drawn or pasted onto the canvas (ibid.). Perhaps the most well-known group to use this method was the Bambanani women's group, whose work was disseminated within the community and online, with the intention of creating political pressure on the government to provide antiretroviral medication to the population (MacGREGOR & MILLS, 2011). Thus body-mapping has therapeutic, artistic and political roots. [2]
Body-mapping has since been used as a research method (GASTALDO, MAGALHÃES, CARRASCO & DAVY, 2012), therapeutic intervention, and community development tool, in educational (EBERSÖHN, 2015; FERREIRA, EBERSÖHN & McCALLAGHAN, 2010), labor (MITCHELL, 2006a), psychological trauma (SANTEN, 2014, 2015), psychological assessment (EBERSÖHN, FERREIRA, VAN DER WALT & MOEN, 2016), health-related (LUDLOW, 2014; ORCHARD, SMITH, MICHELOW, SALTERS & HOGG, 2014; STEVENS & LE ROUX, 2011) and planning (SWEET & ORTIZ ESCALANTE, 2015) contexts, with varying degrees of a social justice agenda. [3]
Body-mapping possesses certain attributes, rendering it uniquely suited to particular research projects. It has 1. a strong social justice history and is intended to be therapeutic, with some participants confirming beneficial effects (NÖSTLINGER et al., 2015). It involves 2. visual stimuli and an arts-based, collaborative, reflective process, which encourages embodied awareness. It is also used as 3. a knowledge translation strategy, that is, to both produce and disseminate empirical research. These aspects of body-mapping are discussed in Section 2 below. Section 3 describes the purpose of the study. The method, including search strategy, data extraction and data evaluation, is detailed in Section 4. Results are reported in Section 5. This includes a detailed numerical summary and thematic analysis. Results are discussed in Section 6, with benefits and potential pitfalls of the use of body-mapping, as well as suggestions for future use. [4]
Body-mapping has its roots in political activism, privileging and making visible otherwise oppressed or obscured perspectives. It provides a means of representing social relationships and processes through body-maps and first person narratives testimonios (GASTALDO et al., 2012). In cases where the phenomenon in question is associated with stigma in the community, body-mapping facilitates participants reclaiming or creating a preferred view of the body, thus bringing into question negative assumptions inherent in dominant narratives or ways of seeing. This notion resonates with narrative therapy approaches (BAMBERG & ANDREWS, 2004; EPSTON, 1999), postcolonial and feminist thought (LEWIS & MILLS, 2003), and the idea of centralizing bodies that are usually hidden or relegated to the margins of society (RICE, CHANDLER, HARRISON, LIDDIARD & FERRARI, 2015). Finally, it is important to be mindful of power imbalances within the research process and attempt to mitigate these as much as possible. [5]
Body-mapping draws participants' attention to their bodies and embodied experience, encouraging awareness and reflection on that embodied experience (GASTALDO et al., 2012; SOLOMON, 2002). This contrasts with other research methods, which tend to neglect bodily or sensory dimensions of experience. For example, as noted by MASON (2006), when a researcher enquires about family relationships, they seldom characterize it in physical terms: movements in relation to each other (touch, activities such as dancing or eating together, or physical assistance with activities of daily living), smells associated with that person (perfume, cooking, the smell of a house or place), or where emotion is felt in the body. This tendency to neglect awareness of the body is by no means unique to the research process, with mind-body dualism permeating Western culture and ways of being and knowing (CRAWFORD, 2010). Indeed, a similar critique has been made of talking therapies, especially in relation to trauma (ibid., see also HERMAN, 2015, VAN DER KOLK, 2015). The continuation of mind-body dualism within a research context is therefore unsurprising. We do not by any means suggest that this aspect of traditional qualitative and quantitative research diminishes their value. However, we argue that it may be fruitful to consider what using body-mapping (which encourages visual processing and/or embodied awareness) offers in terms of access to information which would otherwise be overlooked or rendered invisible. This is particularly relevant when research seeks to understand aspects of an individual's health, which directly concerns embodied experience (CREGAN, 2006; DeMELLO, 2014). [6]
2.3 Knowledge production and translation
Knowledge translation includes knowledge creation as well as knowledge dissemination, with knowledge creation strategies being intimately linked and at times inseparable from dissemination strategies (e.g., BAKER, WILLINSKY & BOYDELL, 2015; BOYDELL, 2011a, 2011b; BOYDELL et al., 2012a; PARSONS & BOYDELL, 2012). Qualitative methods have traditionally been focused on verbal forms of information gathering (via an interview or focus group) (TOLES & BARROSO, 2014) while neglecting visual or embodied research methods and analysis, which are a more recent development (GOUGH & DEATRICK, 2015). Proponents of visual methods and arts-based methods more generally argue that their use facilitates deeper reflection and evokes different information than verbal interview methods alone (HARPER, 2002; WEBER, 2008). Engaging in a creative process during data collection allows access to aspects of experience not readily accessible through interviews, eliciting rich information (BOYDELL et al., 2012a; CORNWALL, 1992). Participants have an active role in the research process, making decisions about how to represent their experience in a highly personalized manner (PARSONS & BOYDELL, 2012). As the process of producing artwork typically takes longer than a verbal interview, it also encourages participants to linger longer, reflecting more deeply on the research topic (BAGNOLI, 2009). This resonates with the narrative therapy practice of "loitering with intent" (e.g., WHITE, 2007; WHITE & EPSTON, 1990). Visual, arts-based methods may be helpful in terms of engaging children and adolescents in research and privileging their perspectives (BAGNOLI, 2009). Similarly, as visual methods rely less on language to communicate than the traditional interview or focus group, they can be used in cases where participants have limited literacy, or where there are language barriers between the research team and participant (ibid.). In both instances, visual, arts-based methods have the potential to minimize power imbalances between researcher and participant, thereby producing more culturally and context-sensitive information (HUSS, KAUFMAN, AVGAR & SHOUKER, 2015). The use of arts in research and dissemination allows for participation in research and renders dissemination of research findings more accessible to the broader community, outside of academia (BARNDT, 2008; BOYDELL et al., 2012a). [7]
Arts-based knowledge translation can be utilized whether or not an artistic product has been created through data collection. For example, in the case of data collected by interview, arts-based means of communicating this data can be applied, however, it requires additional work in terms of conceptualizing how to best represent such data through art and the creative process required to produce artwork. In contrast, the product of a body-mapping workshop is a large work of art with a first person narrative and guide to represent elements of the body-map. While arts-based research continues to grow in popularity as a means of data collection and dissemination (HODGINS & BOYDELL, 2014), most work focuses on photography and drama, with less in found poetry, dance, and body-mapping (PARSONS & BOYDELL, 2012). Body-mapping lends itself well to knowledge translation not only because it involves the production of artwork that is readily available to display, but also due to participants' desire to communicate their stories to others (BOYDELL et al., 2012a; CONRAD & SINNER, 2015). [8]
Body-mapping holds promise in research, therapeutic and community development contexts. However, there is currently no review of published academic literature outlining the ways in which it has been used. The purpose of this study is to systematically identify and synthesize current published literature on the use of body-mapping, examine the contributions of body-mapping to date, and provide recommendations for future use. Although primarily focused on its application in a research context, the nature of body-mapping means that it is often therapeutic or contributes to community development. Consequently, all body-mapping work published in academic journals is reviewed, rather than limiting it solely to research articles. [9]
The objective of the search strategy employed was to identify all published literature using body-mapping. After a preliminary search and consultation with a research librarian (with information science training), "body map*2)" as a key word was identified as the most appropriate search strategy. No time limit or specification for the type of text (article, book) was specified. This search strategy ensured that all relevant articles were captured in the search. The following 10 electronic databases were included: Medline, EMBASE, Global Health, CINAHL, Informit Health Collection, ProQuest Social Sciences, Scopus, Web of Science, ERIC and PsychInfo. All articles located were exported to the reference management system EndNote. The broad capture of the search strategy returned many irrelevant articles, however, ensured that all pertinent articles were identified.
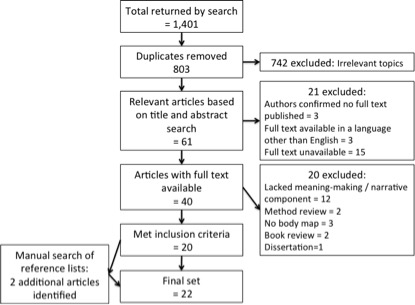
Figure 1: Flow chart of process utilized to identify relevant articles that met inclusion criteria [10]
In total, 1,401 articles were exported, with 803 remaining after duplicates were removed. Following this, the first researcher (ADJ) conducted a title and abstract search, deleting all irrelevant articles, leaving 61 articles, which required further investigation. Of these, the full text was unavailable for 21. The main reason for this appeared to be that no full text was published (confirmed by 3 authors of the texts in question, who responded to our e-mail query) or that the full text was available in a language other than English (3). After eliminating 21 articles for these reasons, 40 articles remained. The first and second researchers (ADJ and AT) independently evaluated each article for inclusion based on the following criteria: 1. a whole-body body-map is included (depictions of a specific body part excluded) and 2. include meaning-making by the participant of the body-map, ideally in the form of a first-person narrative. Inter-rater agreement on inclusion of the 40 articles was 95%. The fourth researcher (KB) resolved disagreements between the two evaluators. As a result of this process, 20 articles remained. A manual search of the reference lists revealed two further articles, which met inclusion criteria, producing a final total of 22 articles. Grey literature was excluded from the review. A preliminary, unsystematic search revealed that most of the unpublished body-mapping projects described HIV/AIDS body-mapping workshops. [11]
Study data was extracted using a standard form and entered into an Excel spread sheet in tabular form. Data was extracted by one reviewer and checked for accuracy and completeness by a second reviewer. Data extracted included: author, country of primary author, topic investigated, study aim, methods, participant characteristics, and study results. Comments on body-mapping as a method and participant experiences were also documented. [12]
4.3 Evaluation of adherence to operationalized definition of body-mapping
Body-mapping as developed by SOLOMON's (2002) guidelines include three elements: 1. a visual body-map, 2. a testimonio,3) or short first-person narrative, and, 3. a key to interpret the symbols and slogans on the body-map. As the aim of this review was to evaluate how body-mapping has been used in published literature to date, articles were not excluded if they did not possess all three elements. Instead, the extent to which the body-mapping process employed emulated that described above was reviewed according to the following criteria, with a point awarded for each element present and out of a maximum ten points:
There is a life-sized body-map.
It is created by tracing around the participant, or if this was inappropriate, around the researcher.
It refers to the individual participant.
It is decorated and drawn on during a creative process, which
includes meaning-making, for example in the form of reflection or qualitative interview (not developed into a narrative).
The meaning-making is in the form of a first-person narrative (testimonio), and
the body-map includes symbols, and
personal slogans.
It involves witnessing or reflection on the individual's body-map by others during the process of body-mapping.
It is disseminated through display in a public space. [13]
In cases where it was not possible to determine the presence of these elements within the published text, an attempt was made to contact the first author to request more information. Of the eight authors contacted, six responded. Where an element could not be confirmed, it was considered absent. The rating produced by this evaluation is indicative of the extent to which the method employed is similar to our operationalization of body-mapping, and not a comment on the overall quality of the research or practice described. [14]
5.1 Descriptive numerical summary
A summary of the 22 included articles representing 19 discrete studies is presented in Table 1. The year of publication ranged from 1992 to 2015. In terms of countries where body-mapping was conducted, Canada (n=7) and South Africa (n=4) featured prominently, followed by Australia (n=3), with remaining projects in the United Kingdom, Philippines, Mexico, and Belgium. One study spanned the United States, Mexico and Spain (SWEET & ORTIZ ESCALANTE, 2015). Of the 19 original studies, 15 incorporated the actual visual images of the body-maps in the article or book chapter.

Figure 2: Geographical location of body-mapping articles included [15]
HIV/AIDS was the most common domain to be researched using body-mapping within the published academic literature (n=6/19). Body-mapping has also commonly been used for a broad range of other health-related areas, including sexual health (n=2), child health (n=2), trauma (n=2), grief (n=1), domestic violence (n=1), undocumented workers (n=1), teacher training (n=1), and end-stage renal disease (n=1). Given how well suited body-mapping is to examining phenomena related to the body, health and relevant social processes, these results are perhaps unsurprising. However, interestingly, body-mapping has also been used to examine the embodied experience of social space, place and belonging (n=1). Although a departure from health research, body-mapping appeared to be very well-suited to this type of investigation, allowing an enriched, embodied understanding of topics usually investigated by more traditional, quantitative means (for example, a safety audit). [16]
The extent to which the body-mapping described adhered to our operationalization varied considerably, from 4 to 10 out of 10. The use of body-mapping ranged from literal descriptions of the effects of work to more complex examinations which included the meaning(s) that participants ascribed to embodied experience and the use of body-maps as tools for empowerment, education or advocacy. [17]
It is of note that some academic articles discussed existing community HIV/AIDS body-mapping projects from a particular theoretical perspective, rather than presenting original research. In addition to articles identified by the review, it is also pertinent to note work not included in the published academic literature. Several body-mapping projects were mentioned in-text with no associated academic article. GASTALDO and colleagues' work on body-mapping with undocumented workers (GASTALDO, CARRASCO & MAGALHÃES, 2013), the Men's Body Mapping Project4) with long-term survivors of HIV/AIDS (FLICKER et al., 2015), and the Art2be project for people with HIV/AIDS in Kenya are prominent examples of body-mapping projects with no or limited representation in academic literature.
Table 1: Summary of body-mapping articles included. Click here to download the PDF file.
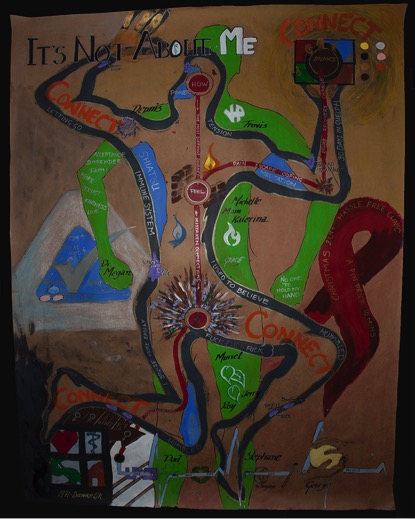
Figure 3: Example of a body-map created by a participant in ORCHARD et al.'s (2014, p.337) research, reproduced with permission
from MaryAnn Liebert publishing. [18]
Upon considering the various uses of body-mapping across the review, several sometimes overlapping themes emerged. Body-mapping was used: 1. as a means of sharing stories via research co-production; 2. for political advocacy; 3. for communication/installation; 4. as a teaching tool or for educative purposes; 5. for planning; 6. as a child-centered method; and finally, 7. for therapy or healing. Due to the nature of body-mapping, it was often not possible to define its use in any given project as falling into only one of these themes. For example, while it was explicitly defined as an arts-based technique for facilitating story-telling in STEVENS & LE ROUX's (2011) work with women who had undergone forced sterilization, it is also more than likely that the process, although potentially emotionally confronting, was of therapeutic benefit for participants. Upon contacting the author, it was clear that the women's stories had been used for advocacy and were used for a political agenda. Similarly, body-maps produced with a political agenda in mind (MacGREGOR, 2009; MacGREGOR & MILLS, 2011) appear to have had therapeutic benefits. In turn, those created primarily as research co-production may have engendered a political intention, for example, to become involved in consumer advocacy, in some participants. Each article was considered along the dimensions described, with results displayed in Table 2.
Table 2: Summary of uses of body-mapping across articles. Click here to download the PDF file [19]
5.2.1 Body-mapping as a means of sharing stories; research co-production
Body-mapping is often used as a means of visual story-telling. The large majority of articles involved body-mapping as story-telling and research co-production, with the exception of those focused on describing body-mapping as a therapeutic intervention (CRAWFORD, 2010; HEMMINGS, 1995; SANTEN, 2014, 2015). As the research knowledge produced is created through storytelling, and the stories are through the research process, these aspects are considered inseparable and discussed as one theme. Through body-mapping, participants engage in creation of data in a creative manner not possible when conducting surveys or interviews (ORCHARD et al., 2014). This mitigates the imbalance in power between researcher and participant, whereby the researcher decides upon questions, which are posed to participant. Body-mapping is therefore a useful method to use with marginalized or vulnerable people. For example, it may mitigate the influence of adult researcher perspectives on children's experiences (MITCHELL, 2006a, 2006b), create a means and context for participants, who may feel disempowered or experience language barriers, to communicate their experiences (NÖSTLINGER et al., 2015) and encourage personalized meanings to emerge, sometimes communicated in visual metaphors (HORNE, 2011). The process of body-mapping allows for a deeper level of reflection on experience than a shorter, verbally-based interview and is therefore likely to facilitate the emergence of richer information. This is alluded to in participants' experiences of surprise at how much information comes to mind during body-mapping and can be depicted on their body-maps (SWEET & ORTIZ ESCALANTE, 2015). In body-mapping, while researchers still guide the process, participants have a greater degree of influence on the data created and the initial interpretation of this data via their testimonios. They make decisions about what colors to use, how to depict themselves, what symbols and slogans to draw and how their body-map will be used. Given the personal nature of body-mapping and investment in their creations, participants are naturally more likely to be included in discussions concerning dissemination of research findings. Thus they are more involved in critical decision-making about the research from production to knowledge translation. [20]
5.2.2 Body-mapping as political advocacy
Body-mapping can be used to advocate for people on a political level and for social change. First, the process itself creates a respectful space where participants' views and experiences are privileged. It renders visible the experiences and perspectives of people whose views are often not sought or marginalized in society. Body-mapping can have an empowering effect, with some participants becoming involved in activism or as expert educators (e.g., MacGREGOR & MILLS, 2011). Second, publishing body-maps, testimonios and other research findings in academic journals or displaying them in a public space ensures that their experiences are better understood by the general public. This can influence policy through pressure from the general public to address a particular issue, or by communicating effectively with key policy-makers. Often the spaces in which body-maps were displayed are indicative of the artists' and researchers' intentions to influence policies or practices. For example, body-maps of HIV positive people were displayed at a conference marking ten years following the end of apartheid. The ongoing effects of HIV on their bodies were discussed as markers of inequality, with the provision of affordable medication being slowly and inefficiently implemented (MacGREGOR, 2009) and the disproportionate effect on poor people of African ethnicities (HORNE, 2011). Similarly, the body-maps of women who had undergone forced sterilization were used locally at a United Nations conference for advocacy purposes, and were included in documentation for country reports (STEVENS, personal communication, October 22, 2015). In keeping with MacGREGOR and MILLS' (2011) work, GAMLIN's (2011) body-mapping research on the effects of agricultural labor on children's bodies provides evidence of a gap between policy and implementation. MITCHELL's (2006a) research regarding children's perspectives on health and illness likewise brings relationships of inequality to the foreground. Specifically, MITCHELL (2006a) notes the dismissal of children's perspectives by adults in the community, broader inequalities between the participants' impoverished living conditions compared to more affluent communities, and a history of Western notions of health being imposed upon Filipino communities. GASTALDO et al. (2013) made subversive use of the body-maps produced by undocumented workers by displaying them at Toronto City Hall, a very public space in a large metropolitan city. LU and YUEN (2012)'s participants also displayed their body-maps, representing embodied experiences of domestic violence and healing, in a local art exhibition. Finally, SWEET and ORTIZ ESCALANTE (2015) do not specifically mention displaying maps in a public space, however, they suggest that body-maps can be used to raise awareness of gender violence issues. They also advocated for their inclusion in urban safety audits. Finally, as their workshops were conducted with planners, it is possible that participants mentioned the issue of gender violence in their respective workplaces after participating in the body-mapping workshop. [21]
5.2.3 Body-mapping as communication/installation
All articles which dealt with the lived experience of HIV/AIDS and the related issue of forced sterilization also involved a public display of body-maps through an installation or exhibition, with some also available on a website (BRETT-MacLEAN, 2009; HORNE, 2011; MacGREGOR, 2009; MacGREGOR & MILLS, 2011; NÖSTLINGER, et al., 2015; STEVENS & LE ROUX, 2011). A public art exhibition was a significant part of VINCENT's (2014) work on embodied experience of place, identity and belonging in relation to physical locations, LU and YUEN's (2012) work on women's experiences of healing after domestic violence, and GASTALDO et al.'s (2013) examination of the experience of undocumented workers. MITCHELL's (2006a) body-mapping work with children living in an impoverished environment was viewed by adults informally during the drawing process, rather than being displayed in a formal exhibition space. CHENHALL, SENIOR and colleagues' work in the area of youth sexual health (CHENHALL, DAVISON, FITZ, PEARSE & SENIOR, 2013; SENIOR, HELMER, CHENHALL & BURBANK, 2014) was presented at academic conferences (personal communication). LUDLOW's (2014) work with patients with end-stage renal disease, GAMLIN's (2011) examination of agricultural labor on children, and GRIFFIN's (2011) work with trainee teachers were not publically exhibited (although trainee teachers had an opportunity to view each other's work). Apart from LU and YUEN's (2012) work, articles reporting on work wherein body-mapping was used for a primarily therapeutic purpose did not include installation or communicative aspects beyond publication of the method in a book or journal (CRAWFORD, 2010; HEMMINGS, 1995; SANTEN, 2014, 2015). [22]
5.2.4 Body-mapping as a teaching tool / education
A minority of the articles reviewed used body-mapping for education purposes. Research on sexual health with adolescents in Australia (CHENHALL et al., 2013; SENIOR et al., 2014) utilized generic female or male body-maps that were filled in through a collaborative process, with participants suggesting details to enrich the narrative accompanying the image. While the primary purpose was to examine adolescents' understandings and experiences of issues related to sexual health, people knowledgeable in this area were present and answered questions posed by participants. LUDLOW (2014) noted the potential use of body-mapping with patients receiving hemodialysis therapy to educate healthcare professionals about their experiences and noted that this occurred naturally during the course of the project, with patients sharing their body-maps with nurses and physicians. Finally, GRIFFIN (2011) incorporated body-mapping into teacher training education for music teacher candidates. It is of note that in all four projects, the interaction between participants and the researcher was collaborative, rather than a "top-down" communication in which hierarchy is emphasized. This applies both to body-mapping as a research process as well as an educational approach. [23]
5.2.5 Body-mapping for examining embodied experience in physical space
Both SWEET and ORTIZ ESCALANTE (2015) and VINCENT (2014)'s work utilized body-mapping to examine embodied experience of physical space. In the former, the focus on inquiry was on women's experiences of violence, fear and safety in urban environments, with a suggestion that the individualized, experience-near description be included in city planning and safety audits. The latter employed body-mapping to explore identity, place and belonging. Although not often utilized for this purpose, body-mapping is well-suited to examining people's embodied experience in relation to the physical world. For example, people's relationship to nature generally, or the embodied experiences of those with particular relationships to the natural world such as an oceanographer, horticulturalist, or farmer; or those who regularly perform particular actions within a given physical context, such as those required by a dancer, jockey, yoga instructor, or physiotherapist, could be effectively explored using body-mapping. Resonances of place in emotions felt in the body can likewise be richly described and reflected upon using body-mapping. [24]
5.2.6 Body-mapping as child/adolescent centered method
Body-mapping was favored for use with children and adolescents as it avoids imposing adult conceptions of the topic being examined (CHENHALL et al., 2013; GAMLIN, 2011; MITCHELL, 2006a, 2006b; SENIOR et al., 2014). In the context of therapy, the use of a creative visual process appears to be helpful for children for several reasons. Drawing or painting activities are likely to be familiar and therefore less anxiety-provoking to children, who are likely to have been exposed to similar tasks at home or at school (HEMMINGS, 1995). The age and developmental stage of child is also relevant, with body-mapping offering a more accessible means of depicting events that are difficult to verbalize (HEMMINGS, 1995; SANTEN, 2014, 2015). [25]
5.2.7 Body-mapping as therapy/healing
In a therapeutic context, body-mapping was acknowledged as a useful therapeutic tool for treating people suffering the psychological effects of trauma (CRAWFORD, 2010; SANTEN, 2014, 2015). HEMMINGS (1995) emphasized the need to establish a safe environment and therapeutic relationship and to consider child/adolescent clients' history before embarking on the body-mapping process. A small but significant proportion of people who experience trauma develop Post Traumatic Stress Disorder, which involves physiological hyperarousal, emotional numbing, re-experiencing the event and avoidance of stimuli associated with the event (FOA, KEANE & FRIEDMAN, 2000). Memories of such experiences are not recalled at will in the form of a complete, coherent memory, instead intruding into consciousness in the form of fragmented visual, auditory, olfactory or tactile sensory memories (VAN DER KOLK, 2015). Trauma also affects the body, with elevated physiological arousal, and altered stress response, including changes to brain structure (FOA et al., 2000; VAN DER KOLK, 2015). The intimate connection between trauma and the body is reflected in metaphors of "inscription" of trauma onto the body. It is the observation of disconnection between experience, memory, self and body that has led some therapists to explore body-mapping as a means of treating trauma (CRAWFORD, 2010). This theme was apparent in the articles reviewed, with body-mapping identified as a helpful means of connecting people to the embodied memory of trauma, which may be inaccessible by other means (CRAWFORD, 2010; SANTEN, 2014, 2015). It was also suggested as a tool to remain attuned to patients' emotions, in that it encourages them to remain connected to a felt, embodied sense of their emotions (rather than dissociating) and to facilitate communication with the therapist about their emotional experiences in the moment (SANTEN, 2014, 2015). Body-mapping can be used to assist clients in communicating their emotions by encouraging them to remain aware of the felt sense of emotion in their bodies and providing a means of communicating this to the therapist, who is able to adjust the pace and intensity of therapy and provide support as appropriate. [26]
In addition to body-mapping conducted with therapeutic benefit as the primary aim, several other authors also noted that their participants mentioned therapeutic benefits. This included an increased awareness and ability to communicate the richness of one's life story, including bodily, individual and societal processes (BRETT-MacLEAN, 2009; GRIFFIN, 2011; ORCHARD et al., 2014), increasing participants' sense of confidence in being able to communicate their health status to others, and developing more effective ways of coping with a health issue (NÖSTLINGER et al., 2015) and building confidence in one's strengths and capacity to contribute (GRIFFIN, 2011). Body-mapping was reported to empower participants through allowing them to reconnect with their strengths and to see themselves as a whole person, with experiences of disease or violence being only one part of their life history (BRETT-MacLEAN, 2009). This is in contrast to dominant narratives of shame or stigma subsuming the person's preferred identity and strengths (BRETT-MacLEAN, 2009; FRANK, 2010). Implicit in such observations of body-mapping is that personal healing overlaps with the socio-political realm, wherein dominant stories are established and retold within a larger socio-political context. Body-mapping was understood to open up, air, allow to breathe and thicken alternative, more helpful narratives of self (WHITE & EPSTON, 1990) with implications for how participants interact with others and an imperative for political or social change. [27]
5.3 Reflections on the use of body-mapping
5.3.1 Benefits of body-mapping to participants
Several articles identified the reported or perceived benefit of body-mapping to participants. These included: 1. developing a richer awareness and thickening of their preferred life narrative (WHITE & EPSTON, 1990); 2. learning to appreciate supportive others and sources of personal power; 3. encouraging an intent to engage in consumer advocacy and/or actions to reduce stigma; 4. enjoying the body-mapping process; 5. facilitating access to process and content unavailable through verbal means alone; 6. encouraging integration of experiences into a coherent sense of self; 7. improving self-esteem; 8. empowering participants; 9. providing participants with an active role in data creation and interpretation; and 10. avoiding imposing the researcher's or broader societal or cultural views onto participants' experience, particularly in the case of research with children or adolescents (BRETT-MacLEAN, 2009; CHENHALL et al., 2013; CRAWFORD, 2010; GAMLIN, 2011; GASTALDO et al., 2013; NÖSTLINGER et al., 2015). [28]
5.3.2 Appropriateness of body-mapping to examine social relationships / processes
Body-maps are regarded as an effective means of depicting social processes and relationships, both within the image and testimonio, as well as through installations in public spaces. Body-maps have the capacity to represent symbolically the ways in which interactions with others and cultural meanings are inscribed and performed through the body, and in turn, how our bodies are the mode through which we interpret the behavior of social others (ERICKSON, 2014). Body-maps are therefore an appropriate way to examine interpersonal space and social meanings. As noted by BLAKESEE and BLAKESEE, "your self does not end where your flesh ends, but suffuses and blends with the world, including other beings" (2008, p.3). In addition to being an appropriate process and product to represent such relationships and processes, body-maps are also amenable to communicating findings to others. Accordingly, body-maps were often displayed in a public space or online as a means of reducing stigma, increasing awareness and giving voice to perspectives that would otherwise remain un-seen/heard. [29]
5.3.3 Suggested future uses and lessons learned
Suggested future uses for body-mapping included use as a tool to supplement medical assessment, diagnosis and communication (BRETT-MacLEAN, 2009; LUDLOW, 2014) and as a strategy to understand women's embodied experiences in relation to safety in urban environments (SWEET & ORTIZ ESCALANTE, 2015). Several authors noted issues to take into account when using body-mapping, including: 1. initial informed consent and discussion of ethics; 2. adjusting the nature of facilitator questions in accordance with the level of trust between group members and the facilitator (ibid.); 3. ongoing negotiation of consent, particularly in relation to participants' emotional state, how images will be used and issue of anonymity (GASTALDO et al., 2012); and 4. considering the context of production and consumption of body-maps (MITCHELL, 2006b). [30]
6.1 Benefits and potential pitfalls of body-mapping
Body-mapping is visual, encourages connection to embodied experience, and involves a creative and reflexive process that is often beneficial for participants and amenable to knowledge translation. CORNWALL (1992), in her exploration of Southern Zimbabwean women's understandings of their sexual and reproductive health, noted the advantage of visual methods in avoiding the imposition of a particular cultural understanding onto others, thereby excluding their definitions. Similarly, visual methods were considered useful with children and adolescents (CHENHALL et al., 2013; GAMLIN, 2011; MITCHELL, 2006a, 2006b & SENIOR et al., 2014) and to overcome language barriers between researchers and participants (GAMLIN, 2011; MITCHELL, 2006a, 2006b). The majority of available information based on informal participant reports across articles indicated multiple benefits to participants (BRETT-MacLEAN, 2009; CRAWFORD, 2010; CHENHALL et al., 2013). Participants reported a heightened awareness of the richness of their life histories, thickening of preferred stories or alternate ways of interpreting their experiences, and an increased sense of self-worth, power and agency. [31]
Nonetheless, MITCHELL (2006b) noted that there is scope for negative consequences to participants and a need to consider the context of production and dissemination of body-maps and associated information. As pointed out by LENETTE and BODDY (2013) in relation to Digital Story-telling, while the participants in the studies reviewed appear to have found body-mapping appropriate and helpful, it is possible that this is not the case for all people. Indeed, although digital stories, like body-mapping, are generally perceived as enjoyable or helpful for participants, it should not be assumed that this is the case for all people. Some participants may experience a level of intrusiveness or burden (ibid.). It is also possible that there is a selection bias in such studies, whereby people for whom it may be unhelpful tend to decline to participate. It is also worth bearing in mind that participants may feel pressure to produce a story that ends on a positive note (BOYDELL et al., 2015). Similarly, in terms of dissemination, there may be some cases where public display of body-maps is inappropriate or where appropriate permission to do so is difficult to obtain. This is most likely to be relevant when working with people who are vulnerable due to physical or psychological health difficulties, or social inequality. The ethical concerns in performing or displaying difficult experiences through art has been explored by BOYDELL et al. (2012b). The ethics of body-mapping including queries regarding: 1. who "owns" the artwork produced; 2. representation and multiple, divergent interpretations of artwork and whose interpretation is privileged; 3. informed consent and reconsidering confidentiality and anonymity given that some participants wish to include identifying details, and longer-term implications of this; 4. the increased likelihood of arts-based methods evoking strong and sometimes distressing emotions; and 5. the tension between research and aesthetic principles in defining the quality of artwork (BOYDELL et al., 2012b). We recommend that these issues be borne in mind in relation to each individual body-mapping project and context. [32]
Several philosophers have argued for the centrality of the body in human experience (f.e., MERLEAU-PONTY, 1962 [1945]). Rather than interfering with our ability to perceive reality or truth, our bodies define how we are in the world. If it were possible to be conscious without a body, this would represent a way of being distinctly different to embodied, human experience. The notion of embodied consciousness is contrary to a dualistic understanding of the mind and body, whereby the body is viewed as an object, merely transport for the mind, rather than intimately intertwined with it. This shift in thinking is concisely expressed by MERLEAU-PONTY's point that we do not have bodies, we are our bodies. This gestures toward the finitude of our bodies, with that which is knowable apprehended through embodied existence, and the unknown lying beyond our horizons (BARTHOLD, 2015; GADAMER, 1992 [1960]; TODRES, 2007). Further, as our perception is always already embodied, it is not possible to evaluate an object in the world from a neutral or objective stance (CARMAN, 1999; MERLEAU-PONTY, 1962 [1945]). Rather, one is oriented toward an experience based on one's previous experiences and informed by one's historical and social situation (BARTHOLD, 2015; GADAMER, 1992 [1960]). Thus our bodies are not neutral, but rather socially and historically situated and inscribed. [33]
The notion of embodied consciousness has been influential and applied to various contexts, including health services research (GRAY & KONTOS, 2015; HAMINGTON, 2004; WILDE, 2003). Drawing on strands of thought from GADAMER, HEIDEGGER and MERLEAU-PONTY, TODRES (2007) describes the body's involvement in unfolding of knowledge through the embodied, lived interaction between researcher and participant. The body is understood as being intimately involved in a process whereby aspects of the "unknown" or "more" that is always present just beyond our knowledge horizons, can unfold and become articulated, in an ongoing play between the familiar and unfamiliar. The prosody, tone, volume, pace and timbre of a research interview or therapy session are related to this "play." The semiotics of language—rhythm, tone, pitch and volume—are as essential in producing meaningful speech as the symbolic, logical aspect of language (KRISTEVA, 1980). It is this dynamic, live, responsive quality of experience and knowledge that is missed or made oblique when the body is not considered. [34]
It should be acknowledged that there is a gendered and cultural association implicit in this discussion, with the mind, reason, Western, masculine privileged over the body, intuition/emotion, non-Western and feminine (LENNON, 2014). Feminist critiques of issues of embodiment are beyond the scope of this review, however, are recommended to interested readers (e.g., BORDO, 1993; BUTLER, 1990; DE BEAUVOIR, 2011 [1949]); KRISTEVA, 1980; YOUNG, 2005). Most relevant to this article is the observation that certain ways of knowing appear to be privileged while other (e.g., embodied) ways of knowing are generally not considered important in knowledge production in research. [35]
A similar trend is evident in the therapeutic realm, with an emphasis on embodied experience not commonly incorporated into psychological therapies. There are some exceptions, for example, somatic psychotherapy, meditation-based practices, yoga, Reiki, biofeedback, art and dance/movement therapies all emphasize bodily experience. The evidence for the efficacy of these interventions varies, with stronger evidence for mindfulness, yoga and biofeedback, while research into Reiki and arts-based therapies are in their infancy (ARCHER, BUXTON & SHEFFIELD, 2015; BARNETT, SHALE, ELKINS & FISCHER, 2014; DESVEAUX, LEE, GOLDSTEIN & BROOKS, 2015; GOMES, COGHI & COGHI, 2014; LEE, PITTLER & ERNST, 2008; PASCOE & BAUER, 2015; SCHOENBERG & DAVID, 2014; VAN DER WAART, GIJSEN, DE WILDT & KOREN, 2009). Within a more traditional therapeutic approach, imaginal exposure and imagery rescripting (ARNTZ, TIESEMA & KINDT, 2007), as well as relaxation and breathing techniques (CRAWFORD, 2010), incorporate bodily experience, awareness and intervention. [36]
Body-mapping exhibitions or online representation arguably have a greater impact on social awareness and attitudes, via exhibitions and online presence, than academic articles. The primary aim of such workshops is to be therapeutic and bring about social change. Accordingly, they may be peer-led or run by counselors, therapists, artists or people with a combination of these skills. Group facilitators or members may not view academic journals as being an effective means of achieving their goals. A second observation regarding the results of our review is that given the promise body-mapping holds as a research method, it has not often been used for this purpose. Of those articles where body-mapping was utilized in a research context, the quality of the body-mapping varied and was not always applied to its full potential. This is particularly relevant in regard to a missed opportunity for knowledge translation; often body-maps produced in a research context were not exhibited or used for advocacy. Thus we suggest that researchers could learn from non-research applications of body-mapping, while community-based workshops may wish to consider contributing to the research literature. Of course those involved in community-based workshops would need to apply for ethics approval to conduct research before commencing the workshops, and have an understanding of research methods and design. However, this should be possible to achieve in collaboration with a research team. As is amply demonstrated by several of the articles reviewed, it is possible to achieve therapeutic, artistic, research and social advocacy goals within the same project. [37]
Interestingly, several prolific body-mapping groups and workshops were not represented in the articles returned by our systematic review. It appeared that in many cases, body-mapping workshops were held, often with public exhibitions of the artwork produced; however, no corresponding academic journal articles were published. For example, the artworks produced through the Art2Be body-mapping projects were turned into a traveling exhibition with stops at various locations within Kenya, as well as being exhibited in London and Berlin (Art2be). Similarly, while the Bambanani group is mentioned several times and some articles discussed are based on their work, few report directly on their process and results. However, there is a permanent exhibition of a selection of their works at the Constitutional Court in Johannesburg, South Africa. [38]
It is possible that for those conducting body-mapping in a non-research context, publishing in an academic journal is not perceived to confer many benefits. In addition, workshop facilitators may not have training in academic authorship. Conversely, re-curating body-maps may be challenging for researchers trained in writing about phenomena rather than the practice of display and design. Whatever the reason, there is often a disconnect between research body-mapping and subsequent public display of research products. [39]
6.4 Evolution of mapping the self
A body-map is a document containing an experience by an individual at one instance. In most body-mapping studies and community workshops, a body-map communicates a message such as: "This is who I am, this is my story, and this is what is important to me." Body-mapping, like identity, is socially-constructed, and shaped by recognition of difference (HALL, 1996). How difference is recognized is through the act of giving meaning to identity, specifically self-identity, and identity in relationships, often through the sharing of stories (FRANK, 1995, 2002). The earliest account of body-mapping in the literature is in 1987, describing research conducted in 1985 by MacCORMACK and DRAPER, but arguably, people have been exploring ways to visually represent themselves since the beginning of humanity, such as in cave drawings in Australia, France, South Africa and Spain. [40]
Considering the form of the body-map, and the initial outline, there are many questions that future research can consider. The act of creating a body tracing, versus starting with a blank page and creating a subjective drawing of the self, is worth exploring. Indeed, a body tracing, or outline, is one way for a participant to directly communicate a story about their body because the outline is similar to stamping an image of the body outline onto paper, and then continuing with mapping. A subjective drawing of the self onto a blank page taps into the subconscious, allowing the "mapper" to express what they perceive is an image of themselves, and continue mapping as they would when sharing a testimonio. [41]
A third issue at stake is the size of the map: should the body-map be created at life-size, or is it fine to create a smaller, or larger-than-life body-map and achieve the same health benefits as one would when body-mapping at-size with an outline? Furthermore, curatorial questions arise such as when a participant's body is traced on the floor, and then the map is hung upright on a wall, does the participant experience a sense of disembodiment and disconnection from the map that they created on the floor, versus when viewing it on the wall? Can they talk about and reflect on what they mapped in the same way, compared to looking at it in its original form? Also, if a three-dimensional body-map were to be created, such as in TARR and THOMAS (2011), or in a sculpted or 3-D printed format, does this format offer greater accuracy in representation of the participant's body, or does it create more challenges for both the participant, and the researcher? [42]
Body-mapping with digital technology poses new challenges as opportunities, that have not yet been explored in-depth, in "traditional" body-mapping. When GASTALDO et al. (2013) presented body-maps of migrant workers in public, they were printed on larger-than-life cotton screens. The researchers used Adobe Photoshop to erase and cover personal identifying information to protect the privacy of participants (GASTALDO et al., 2012). This exercise hints at some of the issues involved in using digital technology to create body-maps, which has the potential to store meta-data with date and time documentation, GPS location, address book contact information, and personal contact information of participants. [43]
6.5 Critique of body-mapping as a research method and therapeutic intervention
It has been claimed that body-mapping: 1. elicits different or richer information compared to verbal interview alone; 2. is beneficial to participants; and 3. can be used as an effective knowledge translation tool. While the goals of body-mapping in a therapeutic context are different to body-mapping used in research, there is substantial overlap, with points 1. and 2. above applying to both research and therapeutic contexts. Thus they are discussed together. While there is anecdotal evidence to support these claims, they have not been formally evaluated. Indeed, a similar critique applies to visual methods more generally, with no formal evidence that it provides access to information not available through verbal interview alone. For example, while TARR and THOMAS (2011) noted that dancers recalled more injuries during the qualitative phase of their research than reported on a questionnaire measure, the interview and viewing of 3D "body-maps" were intertwined. It is therefore difficult to confirm whether the 3D body-map elicited any information above and beyond what would have been elicited by the interview alone. A formal comparison of interview alone versus interviews based on a body-mapping process would clarify this issue. To our knowledge, there has been no systematic investigation of information elicited by body-mapping in a therapeutic context compared to traditional methods including clinical interview and questionnaire measures. Similarly, evaluation of participant experiences of body-mapping and efficacy of knowledge translation strategies would be useful. Finally, it should be noted that body-mapping occurs in a social and relational context, which is relevant to participant experiences. For example, as noted by SWEET and ORTIZ ESCALANTE (2015) the depth to which it is appropriate to lead the interview and group body-mapping process depends on the nature of the relationship between participants and researchers, as well as other group members. Similarly, body-mapping used as a research method may be inappropriate for use with people who have experienced trauma. While in a therapeutic context the therapist is likely to be aware of this issue, there may be contexts in which research participants may be distressed by increased awareness of embodied experience. As with any method, awareness of these types of issues and how to manage them safely is an important consideration when employing body-mapping. [44]
6.6 Suggestions for future use
After thirty years of explorations in body-mapping research, a few researchers have developed digital body-mapping systems, primarily as health-based interventional tools for visual communication of pain (TARR & THOMAS, 2011), and as pain monitoring and communication of illness adjustment (LUDLOW, 2014). Following on the recommendation of SOLOMON (2002), when facilitating a body-mapping project for the first time, LUDLOW (2012) designed a tablet body-mapping application to create body maps with the application before facilitating body-mapping sessions in the dialysis unit to learn about the needs of participants in the actual study. [45]
Understanding that "a map can be defined as any scheme that spells out one-to-one correspondences between two different things" (BLAKESLEE & BLAKESLEE, 2008, p.7), what we have learned from the literature on body-mapping with analog approaches (paper and paint, for example) is that the types of body-mapping that participants do informs how they come to understand their health experiences. An "app" will not end the need to explore and communicate health experiences. Researchers approaching the design of a digital body-mapping system need to account for participant needs. [46]
The contemporary concept of technoscience, involving technologies of the everyday, comes out of pragmatism and phenomenology (IHDE, 2009). IHDE sees technologies (emphasis added) as "material cultures within a lifeworld" versus detached, or passive entities that we interact with on a day-to-day basis (p.22). Consequently, using a variety of technologies of the everyday, such as an iPad, laptop, motion sensor, and data projector to create a body-map is a step towards a future technoscientific approach to body-mapping. A few researchers have developed digital body-mapping systems, primarily as health-based interventional tools for visual communication of pain (TARR & THOMAS, 2011). Our third author (BL) developed a prototype of a digital, web-based body-mapping application in June 2011 before facilitating body-mapping sessions in the dialysis unit to learn about the needs of participants in the actual study (2012). The application can be used alone, or in conjunction with face-to-face body-mapping workshops. To our knowledge, it is the first of its kind to be developed. [47]
6.6.2 Global health perspective
KOPLAN et al. (2009) define "global health" as:
"an area for study, research, and practice that places a priority on improving health and achieving equity in health for all people worldwide. Global health emphasises transnational health issues, determinants, and solutions; involves many disciplines within and beyond the health sciences and promotes interdisciplinary collaboration" (p.1995). [48]
We therefore acknowledge the potential of body-mapping in a global health context. Unlike national health, it is a global health intervention because the issues that body-mapping addresses in the literature are health issues that "transcend national boundaries" (p.1994), and affect people around the world, such as HIV/AIDS, pain, reproductive health, and trauma. [49]
For body-mapping to develop as a research method, it needs to grow through collaboration, which is a defining characteristic of global health (BEAGLEHOLE & BONITA, 2010). BOYLE, LEVIN, HATEFI, MADRIZ and SANTOS (2015) regard collaboration as the "grand convergence" healthcare scenario that is a democratizing paradigm shift that brings together low versus high income populations to allocate resources to all. As demonstrated in our review, body-mapping can be used as an interdisciplinary research method across diverse cultures to address critical issues in health and is amenable to sharing information between researchers and with the public—characteristics defined by ABOELELA et al. (2007) as necessary for a global health research method. ORCHARD (personal communication, December 11, 2015) is in the process of developing a systematic means of analyzing body-maps, which may increase their utility in some research contexts. [50]
While in a research context therapeutic benefit is a by-product of the process, it is not the primary aim. However, the characteristics of body-mapping also mean that it can be used as a global health intervention. Based on our review, there is qualitative evidence of therapeutic effects of body-mapping including increased empowerment, self-esteem and hope, and decreased self- and other-generated stigma. It also appears to have a reasonable rationale for use in treatment of trauma (CRAWFORD, 2010; HEMMINGS, 1995; SANTEN, 2014, 2015), although more research is required to confirm its efficacy. Empirical examination of both of these hypotheses would provide further information to allow evaluation of its therapeutic effect, which may demonstrate an evidence-base for its use as a health intervention. [51]
Body-mapping holds promise in educational, research and clinical spheres. It has the potential to be used globally in healthcare and other contexts. More empirically grounded work would strengthen its acceptability in certain research and clinical contexts. We believe this work would be worthwhile given the benefits of body-mapping discussed. It offers an embodied way of knowing and storying the self that is part of a broader interest in bringing the body and arts into focus in research and therapeutic process. [52]
Our thanks to Denise GASTALDO and her colleagues for their work in the field of body-mapping particularly their excellent online guide to facilitating body-mapping sessions. We are also grateful to the many authors who responded to our inquiries with more information about their research.
1) The Lifelong and Memory Box projects were developed as a means of celebrating the lives of HIV positive people and creating a legacy to leave behind for their children and families after their deaths. See for example http://www.capetown.at/letters/mem_box.htm [Accessed: April 13, 2016]. <back>
2) The use of "*" after the first few letters of a word ensures that the search captures all words beginning with these letters. In our case the search captured "body map," "body maps," and "body mapping." <back>
3) To our knowledge, the term "testimonio" was first used by GASTALDO et al. (2012) to refer to the narratives that accompany body-maps. <back>
4) The Men's Body-Mapping Project is a community-based research initiative that encourages people to think differently about HIV; see https://sites.google.com/site/bodymaps/home [Accessed: April 13, 2016]. <back>
Aboelela, Sally W.; Larson, Elaine; Bakken, Suzanne; Carrasquillo, Olveen; Formicola, Allan; Glied, Sally A.; Haas, Janet & Gebbie, Kristine M. (2007). Defining interdisciplinary research: Conclusions from a critical review of the literature. Health Services Research, 42(11), 329-346.
Archer, Stephanie; Buxton, Sarah & Sheffield, David (2015). The effect of creative psychological interventions on psychological outcomes for adult cancer patients: A systematic review of randomised controlled trials. Psycho-Oncology, 24, 1-10.
Arntz, Arnoud; Tiesema, Meike & Kindt, Merel (2007). Treatment of PTSD: A comparison of imaginal exposure with and without imagery rescripting. Journal of Behavior Therapy and Experimental Psychiatry, 38(4), 345-370.
Australian Commission on Safety and Quality in Healthcare (2011). Patient-centred care: Improving quality and safety through partnerships with patients and consumers, http://www.safetyandquality.gov.au/wp-content/uploads/2012/03/PCC_Paper_August.pdf [Accessed: March 4, 2016].
Bagnoli, Anna (2009). Beyond the standard interview: The use of graphic elicitation and arts-based methods. Qualitative Research, 9(5), 547-570.
Baker, Natalie A.; Willinsky, Catherine & Boydell, Katherine M. (2015). Just say know: Engaging young people to explore the link between cannabis and psychosis using creative methods. World Cultural Psychiatry Research Review, 10(3/4), 201-220.
Ball, Susan & Gilligan, Chris (Eds.) (2010). Visualizing migration and social division: Insights from social sciences and the visual arts. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 11(2), http://www.qualitative-research.net/index.php/fqs/issue/view/34 [Accessed: March 20, 2016].
Bamberg, Michael & Andrews, Molly (2004). Considering counter narratives: Narrating, resisting, making sense. Amsterdam: John Benjamins.
Barndt, Deborah (2008). Touching minds and hearts: Community arts as collaborative research. In J. Gary Knowles & Andra L. Cole (Eds.), Handbook of the arts in qualitative research: Perspectives, methodologies, examples and issues (pp.351-362). Thousand Oaks, CA: Sage.
Barnett, Jeremy E. M.; Shale, Allison J.; Elkins, Gary & Fisher, William (2014). Complementary and alternative medicine for psychologists: An essential resource. Washington, DC: American Psychological Association.
Barthold, Lauren Swayne (2015). Hans Georg Gadamer (1900-2002). In James Fieser & Bradley Downdon (Eds.), Internet encyclopaedia of philosophy: A peer reviewed academic resource, http://www.iep.utm.edu/gadamer/ [Accessed: November 18, 2015].
Beaglehole, Robert & Bonita, Ruth (2010). What is global health? NIH Global Health Action, 3, 5142, http://www.globalhealthaction.net/index.php/gha/article/view/5142 [Accessed: March 20, 2016].
Blakesee, Sandra & Blakesee, Matthew (2008). The body has a mind of its own: How body maps in your brain help you do (almost) everything better. New York: Random House.
Bordo, Susan (1993). Unbearable weight: Feminism, Western culture and the body. Berkeley, CA: University of California Press.
Boydell, Katherine M. (2011a). Using performative art to communicate research: Dancing experiences of psychosis. Canadian Theatre Review, 146, 12-17.
Boydell, Katherine M. (2011b). Making sense of collective events: The co-creation of a research-based dance. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 12(1), Art. 5, http://nbn-resolving.de/urn:nbn:de:0114-fqs110155 [Accessed: March 20, 2016].
Boydell, Katherine M.; Gladstone, Brenda M.; Volpe, Tiziana; Allemang, Brooke & Stasiulis, Elaine. (2012a). The production
and dissemination of knowledge: A scoping review of arts-based health research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 13(1), Art. 32,
http://nbn-resolving.de/urn:nbn:de:0114-fqs1201327 [Accessed: March 20, 2016].
Boydell, Katherine M.; Gladstone, Brenda M.; Stasiulis, Elaine; Davidson, Simon; Nadin, Shevaun & Cheng, Chiachen (2015). A participatory approach to examining pathways to mental health in rural communities: using digital storytelling. Paper presented at the Society for Mental Health Research Conference, Brisbane, Australia, December 2, 2015, http://www.smhr2015.com.au [Accessed: December 7, 2015].
Boydell, Katherine M.; Volpe, Tiziana; Cox, Susan; Katz, Arlene; Dow, Reilly; Brunger, Fern; Parsons, Janet; Belliveau, George; Gladstone, Brenda M.; Zlotnik-Shaul, Randi; Cook, Sheila; Kamensek, Otto; Lafreneière, Darquise & Wong, Lisa (2012b). Ethical challenges in arts-based health research. The International Journal of the Creative Arts in Interdisciplinary Practice, 11, http://www.ijcaip.com/archives/IJCAIP-11-paper1.pdf [Accessed: March 4th, 2016].
Boyle, Colin F.; Levin, Carol; Hatefi, Arian; Madriz, Solange & Santos, Nicole (2015). Achieving a "grand convergence" in global health: Modeling the technical inputs, costs, and impacts from 2016 to 2030. PLoS ONE, 10(10), e0140092, http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0140092 [Accessed: March 24th, 2016].
Brett-MacLean, Pamela (2009). Body mapping: Embodying the self living with HIV/AIDS. Canadian Medical Association Journal, 180(7), 740-741, http://www.cmaj.ca/content/180/7/740.full.pdf+html [Accessed: March 24th, 2016].
Brogden, Lace Marie (2010). Double hermeneutic. In Albert J. Mills, Gabrielle Durepos & Elden Wiebe (Eds.), Encyclopedia of case study research (pp.322-324). Thousand Oaks, CA: Sage.
Butler, Judith (1990). Gender trouble: Feminism and the subversion of identity. New York: Routledge.
Byrne, Louise; Happell, Brenda; Welch, Tony & Moxham, Lorna Jane (2013). "Things you can't learn from books": Teaching recovery from a lived experience perspective. International Journal of Mental Health Nursing, 22, 195-204.
Canadian Institute for Health Information (2012). Looking back, looking forward, https://www.cihi.ca/en/hcic2012_conclu_en.pdf [Accessed: March 4, 2016].
Canadian Medical Association (2009). Health care transformation in Canada, http://policybase.cma.ca/dbtw-wpd/PolicyPDF/PD10-05.PDF [Accessed: March 4th, 2016].
Carman, Taylor (1999). The body in Husserl and Merleau-Ponty. Philosophical Topics, 27(2), 205-226.
Chenhall, Richard; Davison, Belinda; Fitz, Joseph; Pearse, Tiffanie & Senior, Kate (2013). Engaging youth in sexual health research: refining a "youth friendly" method in the Northern Territory, Australia. Visual Anthropology Review, 29(2), 123-132.
Christmann, Gabriela B. (2008). The power of photographs of buildings in the Dresden urban discourse: Towards a visual discourse analysis. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 9(3), Art. 11, http://nbn-resolving.de/urn:nbn:de:0114-fqs0803115 [Accessed: February 20, 2016].
Conrad, Diane & Sinner, Anita (2015). Creating together: Participatory, community-based, and collaborative arts practices and scholarship across Canada. Ontario: Wilfrid Laurier University Press.
Cornwall, Andrea (1992). Body mapping in health RRA/PRA. RRA Notes, 16, 69-76, http://pubs.iied.org/pdfs/G01449.pdf [Accessed: October 20, 2015].
Crawford, Alison (2010). If "the body keeps score": Mapping the dissociated body in trauma narrative, intervention and theory. University of Toronto Quarterly, 79(2), 702-719, http://documents.mx/documents/mapping-the-ed-body-in-trauma-narrative-and-intervention.html [Accessed: October 20, 2015].
Cregan, Kate (2006). The sociology of the body: Mapping the abstraction of embodiment. Thousand Oaks, CA: Sage.
Davis, Karen; Schoenbaum, Stephen C. & Audet, Anne-Marie (2005). A 2020 vision of patient-centred primary care. Journal of General Internal Medicine, 20, 953-957, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1490238/ [Accessed: March 4, 2016].
De Beauvoir, Simone (2011 [1949]). The second sex (trans. by C. Borde & S. Malovany-Chevallier). New York: Random House.
DeMello, Margo (2014). Body studies: An introduction. London: Routledge.
Desveaux, Laura; Lee, Annemarie; Goldstein, Roger & Brooks, Dina (2015). Yoga in the management of chronic disease. Medical Care, 53(7), 653-661.
Ebersöhn, Liesel (2015). Body mapping: Life design with groups of youth in high risk and high need settings. In Mary McMahon & Wendy Patton (Eds.), Ideas for career practitioners: Celebrating excellence in career practice (pp.82-89). Brisbane: Australian Academic Press.
Ebersöhn, Liesel; Ferreira, Ronél; van der Walt, Anél & Moen, Melanie (2016). Bodymapping to step into your future: Life design in a context of high risk and high diversity. In Ferreira Ronél (Ed.),Thinking innovatively about psychological assessment in a context of diversity (pp.228-241). Cape Town: Juta.
Epston, David (1999). Co-research: The making of an alternative knowledge. In Dulwich Centre Publications (Eds.), Narrative therapy & community work: A conference collection (pp.137-157). Adelaide: Dulwich Centre Publications, http://uofthenet.org/NPCI/Co-researchDavidEpston.pdf [Accessed: December 20, 2015].
Erickson, Camille (2014). Toward a transnational queer futurity: The photography of Catherine Opie, Zanele Muholi, and Jean Brundrit. Art and Art History Honors Projects, Paper 4, http://digitalcommons.macalester.edu/art_honors/4/ [Accessed: December 20, 2015].
Ferreira, Ronél; Ebersöhn, Liesel & McCallaghan, Malize (2010). The use of body maps by educators fulfilling their pastoral role. Tydskrif vir geesteswetenskappe, 50(2), 197-215, http://www.scielo.org.za/pdf/tvg/v50n2/v50n2a05.pdf [Accessed: October 20, 2015].
Flicker, Sarah; Mykhalovskiy, Eric; Mehes, Mira; Teolis, Cortleigh; Taylor, Darlen & Smith, Tricia (2015). Men's body mapping research project, https://sites.google.com/site/bodymaps/home [Accessed: October 23, 2015].
Foa, Edna B.; Keane, Terence M. & Friedman, Matthew J. (2000). Guidelines for treatment of PTSD. Journal of Traumatic Stress, 13(4), 539-554.
Frank, Arthur W. (1995). The wounded storyteller: Body, illness and ethics. Chicago, IL: The University of Chicago Press.
Frank, Arthur W. (2002). At the will of the body: Reflections on illness. Boston, MA: Houghton Mifflin Harcourt.
Frank, Arthur W. (2010). Letting stories breathe: A socio-narratology. Chicago, IL: The University of Chicago Press.
Gadamer, Hans-Georg (1992 [1960]). Truth and method (2nd ed., trans. by J. Weinsheimer & D.G. Marshall). New York: Crossroad.
Gamlin, Jennie B. (2011). "My eyes are red from looking and looking": Mexican working children's perspectives of how tobacco labour affects their bodies. Vulnerable Children and Youth Studies, 6(4), 339-345.
Gastaldo, Denise; Carrasco, Christine & Magalhães, Liliana (2013). The creation of a mobile workforce: Latin American undocumented workers in the Greater Toronto Area. Encounters, 1(1), 18-32.
Gastaldo, Denise; Magalhães, Liliana; Carrasco, Christine & Davy, Charity (2012). Body-map storytelling as research: Methodological considerations for telling the stories of undocumented workers through body mapping. Facilitator Guide, http://www.migrationhealth.ca/undocumented-workers-ontario/body%20mapping [Accessed: October 10, 2015].
Gomes, July Silveira; Coghi, Marco Fabio & Coghi, Priscila Fernandes (2014). Cardiovascular biofeedback and its applications: Review of literature. Avances en Psicologia Latinoamericana, 32(2), 199-216, http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S1794-47242014000200002 [Accessed: December 10, 2015].
Gough, Brendan & Deatrick, Janet A. (2015). Qualitative health psychology research: Diversity, power and impact. Health Psychology, 34 (4), 289-292.
Gray, Julia & Kontos, Pia (2015). Immersion, embodiment, and imagination: Moving beyond an aesthetic of objectivity in research-informed
performance in health. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 16(2), Art. 29,
http://nbn-resolving.de/urn:nbn:de:0114-fqs1502290 [Accessed: April 7, 2016].
Griffin, Shelley (2011). Tip-toeing past the fear: Becoming a music educator by attending to personal music experiences. In Julian Kitchen, Darlene Ciuffetelli Parker & Debbie Pushor (Eds.), Narrative inquiries into curriculum making in teacher education (pp.69-192). Bingley: Emerald Group Publishing Limited.
Guillemin, Marilys & Drew, Sarah (2010). Questions of process in participant-generated visual methodologies. Visual studies, 25(2), 175-188.
Hall, Stuart (1996). Who needs "identity"? In Stuart Hall & Paul duGay (Eds.), Questions of cultural identity (pp.1-17). London: Sage.
Hamington, Maurice (2004). Embodied care. Urbana: University of Illinois Press.
Harper, Douglas (2002). Talking about pictures: A case for photo elicitation. Visual Studies, 171, 13-26, http://www.nyu.edu/pages/classes/bkg/methods/harper.pdf [Accessed: March 10, 2016].
Harrison, Barbara (2002). Photographic visions and narrative inquiry. Narrative Inquiry, 12(1), 7-111.
Hemmings, Peta (1995). Communicating with children through play. In Susan Smith & Margaret Pennells (Eds.), Interventions with bereaved children (pp.9-23). London: Kingsley Publishers.
Herman, Judith Lewis (2015). Trauma and recovery. New York: Basic Books.
Hodgins, Michael & Boydell, Katherine M. (2014). Interrogating ourselves: Reflections on art-based health research. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 15(1), Art. 10, http://nbn-resolving.de/urn:nbn:de:0114-fqs1401106 [Accessed: March 20, 2016].
Horne, Felicity (2011). Conquering AIDS through narrative: Longlife positive HIV stories. English Studies in Africa, 54(2), 71-87.
Huss, Ephrat; Kaufman, Roni; Avgar, Amos & Shouker, Eytan (2015). Using arts-based research to help visualize community intervention in international aid. International Social Work, 58(5), 673-688.
Ihde, Don (2009). Postphenomenology and technoscience: The Peking university lectures. New York: Suny Press.
Kitson, Alison; Marshall, Amy; Bassett, Katherine & Zeitz, Kathryn (2013). What are the core elements of patient-centred care? A narrative review and synthesis of the literature from health policy, medicine and nursing. Journal of Advanced Nursing, 69(1), 4-15.
Knoblauch, Hubert; Baer, Alejandro; Laurier, Eric; Petschke, Sabine & Schnettler, Bernt (2008). Visual analysis: New developments in the Interpretative Analysis of video and photography. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 9(3), Art. 14, http://nbn-resolving.de/urn:nbn:de:0114-fqs0803148 [Accessed: March 20, 2016].
Koplan, Jeffrey P.; Bond, T. Christopher; Merson, Michael H.; Reddy, K Srinath; Rodriguez, Mario Henry; Sewankambo, Nelson K. & Wasserheit, Judith N. (2009). Towards a common definition of global health. Lancet, 373, 1993-1995, https://www.globalbrigades.org/media/Global_Health_Towards_a_Common_Definitition.pdf [Accessed: March 20, 2016].
Kristeva, Julia (1980). Desire in language: A semiotic approach to literature and art (transl. by T. Gora & A.A. Jardine, ed. by L.S. Roudiez). New York: Columbia University Press.
Lee, Myeong Soo; Pittler, Max H. & Ernst, Edzard (2008). Effects of reiki in clinical practice: A systematic review of randomised controlled trials. International Journal of Clinical Practice, 62(6), 947-954
Lenette, Caroline & Boddy, Jennifer (2013). Visual ethnography and refugee women: Nuanced understandings of lived experience. Qualitative Research Journal, 13(1), 72-89.
Lennon, Kathleen (2014). Feminist perspectives on the body. In Edward N. Zalta (Ed.), The Stanford encyclopedia of philosophy, http://plato.stanford.edu/archives/fall2014/entries/feminist-body [Accessed: November 18, 2015].
Lewis, Reina & Mills, Sarah (2003). Feminist postcolonial theory: A reader. New York: Routledge.
Lu, Lucy & Yuen, Felice (2012). Journey women: Art therapy in a decolonizing framework of practice. The Arts in Psychotherapy, 39, 192-200.
Ludlow, Bryn (2012). Body mapping with geriatric patients receiving daily haemodialysis therapy for end-stage renal disease at Toronto Rehabilitation Institute: A qualitative study. Unpublished Master of Arts Thesis, McMaster University, Hamilton, Canada, https://macsphere.mcmaster.ca/handle/11375/12677/ [Accessed: April 7, 2015].
Ludlow, Bryn (2014). Witnessing: Creating visual research memos about patient experiences of body mapping in a dialysis unit. American Journal of Kidney Diseases, 64(5), xiii-xiv.
MacCormack, Carol P. & Draper, Alizon (1987). Social and cognitive aspects of female sexuality in Jamaica. In Pat Caplan (Ed.), The cultural construction of sexuality (pp.143-165). London: Routledge.
MacGregor, Hayley N. (2009). Mapping the body: Tracing the personal and the political dimensions of HIV/AIDS in Khayelitsha, South Africa. Anthropology & Medicine, 16(1), 85-95.
MacGregor, Hayley N. & Mills, Elizabeth (2011). Framing rights and responsibilities: Accounts of women with a history of AIDS activism. Bio Med Central International Health & Human Rights, 11(S7), 1-11, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3287463/ [Accessed: March 18, 2016].
Mason, Jennifer (2006). Mixing methods in a qualitatively driven way. Qualitative Research, 6(1), 9-25.
Merleau-Ponty, Maurice (1962 [1945]). Phenomenology of perception (transl. by C. Smith). London: Routledge & Kegan Paul.
Mitchell, Lisa M. (2006a). Body and illness: Considering Visayan Filipino children's perspectives within local and global relationships of inequality. Medical Anthropology, 25(4), 331-373.
Mitchell, Lisa M. (2006b). Child-centred? Thinking critically about children's drawings as a visual research method. Visual Anthropology Review, 22(1), 60-73.
Morgan, Jonathan & Bambanani Women's Group (2003). Long life: Positive HIV stories. Cape Town: Double Storey Books.
Nöstlinger, Christiana; Loos, Jasna & Verhoest, Xavier (2015). Coping with HIV in a culture of silence: Results of a body-mapping workshop. AIDS Research and Human Retroviruses, 31(1), 47-48.
Orchard, Treena; Smith, Tricia; Michelow, Warren; Salters, Kate & Hogg, Bob (2014). Imagining adherence: Body mapping research with HIV-positive men and women in Canada. AIDS Research and Human Retroviruses, 30(4), 337-338.
Parsons, Janet A. & Boydell, Katherine M. (2012). Arts-based research and knowledge translation: Some key concerns for health-care professionals. Journal of Interprofessional Care, 1-3.
Pascoe, Michaela C. & Bauer, Isabelle E. (2015). A systematic review of randomised control trials on the effects of yoga on stress measures and mood. Journal of Psychiatric Research, 68, 270-282, http://www.sciencedirect.com/science/article/pii/S002239561500206X [Accessed: March 24, 2016].
Rapport, Frances (2004). Shifting sands in qualitative methodology. In Frances Rapport (Ed.), New qualitative methodologies in health and social care research (pp.1-18). London: Routledge.
Rice, Carla; Chandler, Eliza; Harrison, Elizabeth; Liddiard, Kirsty & Ferrari, Manuela (2015). Project Re*Vision: Disability at the edges of representation. Disability & Society, 30(4), 513-527.
Ring, Nicola; Ritchie, Karen; Mandava, Lakshmi & Jepson Ruth (2011). A guide to synthesising qualitative research for researchers undertaking health technology assessments and systematic reviews. Scottish network for the generation and exchange of knowledge in evidence synthesis, report of scoping meeting, http://www.healthcareimprovementscotland.org/our_work/technologies_and_medicines/programme_resources/synthesising_research.aspx [Accessed: October 18, 2015].
Royal Australian & New Zealand College of Psychiatrists (2014). Position Statement 62: Consumer, family/whānau and carer engagement, https://www.ranzcp.org/Files/Resources/College_Statements/Position_Statements/PS-62-PPC-Consumer-and-Carer-Engagement.aspx [Accessed: April 7, 2016].
Santen, Bart (2014). Into the fear-factory: Connecting with the traumatic core. Person-Centred & Experiential Psychotherapies, 13(2), 75-93.
Santen, Bart (2015). Treating dissociation in traumatized children with body maps. In Cathy Malchiodi (Ed.), Creative interventions with traumatized children (pp.126-149). New York: Guilford Press.
Schoenberg, Poppy L.A. & David, Anthony S. (2014). Biofeedback for psychiatric disorders: A systematic review. Applied Psychophysiology and Biofeedback, 39(2), 109-135.
Senior, Kate; Helmer, Janet; Chenhall, Richard & Burbank, Victoria (2014). "Young, clean and safe?" Young people's perceptions of risk from sexually transmitted infections in regional, rural and remote Australia. Culture, Health & Sexuality, 16(4), 453-466.
Solomon, Jane (2002). "Living with X": A body mapping journey in time of HIV and AIDS. Facilitator's Guide. Psychosocial Wellbeing Series. Johannesburg: REPSSI.
Stevens, Marion & Le Roux, Nicole (2011). A human rights violation: The forced sterilization of HIV positive women. Nursing Update, 35(3), 32-35.
Sweet, Elizabeth L. & Ortiz Escalante, Sara (2015). Bringing bodies into planning: Visceral methods, fear and gender violence. Urban Studies, 52(10), 1826-1845.
Tarr, Jen & Thomas, Helen (2011). Mapping embodiment: Methodologies for representing pain and injury. Qualitative Research, 11(2), 141-157.
Todres, Les (2007). Embodied enquiry: Phenomenological touchstones for research, psychotherapy and spirituality. New York: Palgrave Macmillan.
Toles, Mark & Barroso, Julie (2014). Introduction to qualitative health research. In Geri LoBiondo-Wood & Judith Haber (Eds.), Nursing research: Methods and critical appraisal for evidence-based practice (8th ed., pp.95-108). St. Louis, MI: Mosby, Elsevier.
Van Der Kolk, Bessel (2015). The body keeps the score: Brain, mind, and body in the healing of trauma. New York: Penguin Books.
Van der Waart, Sondra; Gijsen, Violette M.; de Wildt, Saskia N. & Koren, Gideon (2009). A systematic review of the therapeutic effects of Reiki. Journal of Alternative Complementary Medicine, 15(11), 1157-1169.
Vasquez, Gioconda (2004). Body perceptions of HIV and AIDS: The Memory Box Project. Cape Town: Centre for Social Science Research, University of Cape Town, http://cssr.uct.ac.za/sites/cssr.uct.ac.za/files/pubs/wp64.pdf [Accessed: April 12, 2016].
Verma, Jennifer; Peterson, Stephen; Samis, Stephen; Akunov, Nurdin & Graham, Jeffrey (2014). Healthcare priorities in Canada: A backgrounder. Ottawa: Canadian Foundation for Healthcare Improvement, http://www.cfhi-fcass.ca/sf-docs/default-source/documents/harkness-healthcare-priorities-canada-backgrounder-e.pdf [Accessed: March 31, 2016].
Vincent, Rachael (2014). Experiments with bodies in social space: Towards a contemporary understanding of place-based identities at the social history museum. Museum Management and Curatorship, 29(4), 368-390.
Weber, Sandra (2008). Visual images in research. In Gary Knowles & Ardra Cole (Eds.), Handbook of the arts in qualitative research: Perspectives, methodologies, examples, and issues (pp.41-54). Thousand Oaks, CA: Sage.
White, Michael (2007). Maps of narrative practice. New York: W.W. Norton.
White, Michael & Epston, David (1990). Narrative means to therapeutic ends. New York: W.W. Norton.
Wilde, Mary H. (2003). Embodied knowledge in chronic illness and injury. Nursing Inquiry, 10(3), 170-176.
Young, Iris Marion (2005). On female body experience: “Throwing Like a Girl” and other essays. Oxford: Oxford University Press.
Adèle DE JAGER is a research officer at the Black Dog Institute and clinical psychologist in private practice. As part of her doctorate, she employed narrative analysis to investigate the lived experience of recovery in people who hear voices. Results were published in Qualitative Health Research and disseminated by informal means (e.g., pamphlet). Her work at the Black Dog Institute focuses on qualitative research into psychosis and arts-based methods in research and dissemination. She co-facilitates the Sydney Narrative Inquiry Research Group.
Contact:
Adèle de Jager
Black Dog Institute
University of New South Wales
Hospital Road, Randwick, NSW, 2031, Australia
Tel.: (+61) 2 9382 9275
E-mail: a.dejager@blackdog.org.au
URL: http://www.blackdoginstitute.org.au
Anna TEWSON is a writer and research assistant at the Black Dog Institute. She writes poetry and short stories, and enjoys blending elements of the metaphysical with the real. Anna aspires to use the skills learned in her degree to open an all-inclusive space for the public, in which they can tell new and different stories through writing, drama and music. Her work at the Black Dog Institute is centered around arts-based research and dissemination.
Contact:
Anna Tewson
Black Dog Institute
University of New South Wales
Hospital Road, Randwick, NSW, 2031, Australia
Tel.: (+61) 2 9382 9275
E-mail: a.tewson@blackdog.org.au
URL: http://thequarryjournal.com/smothered-anna-tewson/, http://www.blackdoginstitute.org.au
Bryn A. LUDLOW is a second-year doctoral student at York University in the Department of Communication Studies, York & Ryerson Joint Graduate Program in Communication & Culture, Toronto, Canada. In 2012, she completed a Master of Arts degree in health & aging from McMaster University in the Department of Health, Aging & Society, and applied the visual research method of body-mapping in the dialysis unit with five geriatric inpatients to learn about their experiences of receiving daily (six day/week) hemodialysis therapy at Toronto Rehabilitation Institute. Her research and teaching interests specifically address themes of curating in art and science; affect and technology; and visual and health communication.
Contact:
Bryn A. Ludlow
York University
4700 Keele St, Toronto, ON M3J 1P3, Canada
E-mail: bludlow@yorku.ca
URL: http://brynludlow.com
Katherine M. BOYDELL is professor of mental health at the Black Dog Institute, University of New South Wales, Australia. Her research is both methodological and substantive; substantively, it focuses on understanding the complex pathways to care for young people experiencing a first episode of psychosis, the use of new technologies in child and youth mental health, and the "science" of knowledge translation. Methodologically, it focuses on advancing qualitative inquiry, specifically, in the area of arts-based health research. Katherine explores the use of a wide variety of art genres in the creation and dissemination of empirical research, including documentary film, dance, digital storytelling, found poetry, installation art and body mapping. Her work takes a critical perspective and focuses on the theoretical, methodological and ethical challenges of engaging in arts-based health research. She has published more than 100 journal articles and edited a recent text with Bruce FERGUSON titled "Hearing Voices: Qualitative Inquiry in Early Psychosis" (Wilfred Laurier University Press: Ontario, Canada).
Contact:
Katherine M. Boydell
Black Dog Institute
University of New South Wales
Hospital Road, Randwick, NSW, 2031, Australia
Tel.: (+61) 2 9382 8501
E-mail: k.boydell@unsw.edu.au
URL: http://www.katherineboydell.com, http://www.blackdoginstitute.org.au
de Jager, Adèle; Tewson, Anna; Ludlow, Bryn & Boydell, Katherine M. (2016). Embodied Ways of Storying the Self: A Systematic
Review of Body-Mapping [52 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 17(2), Art. 22,
http://nbn-resolving.de/urn:nbn:de:0114-fqs1602225.

Creative Commons Attribution 4.0 International License