Volume 19, No. 2, Art. 3 – May 2018
Body-Map Storytelling as a Health Research Methodology: Blurred Lines Creating Clear Pictures
Denise Gastaldo, Natalia Rivas-Quarneti & Lilian Magalhães
Abstract: In this article we review the literature on body mapping (BM) as an approach to health research in order to systematize recent advancements and to contribute to its development. We conducted a critical narrative synthesis of the literature published until September 2016 guided by two questions: 1. How has BM been utilized in health research? 2. How does BM advance a decolonization agenda? Twenty-seven studies in English, Spanish, and Portuguese were analyzed. Most of them were published between 2011 and 2016 and were conducted in South Africa, Canada, Australia, Brazil, Chile, and USA. They narrate stories of marginalized groups and commonly focus on the social determinants of health. Data generation, analysis, and knowledge mobilization strategies differ considerably. Recent developments show that body mapping is a visual, narrative, and participatory methodology that has several names and is used unevenly by health researchers. Despite its diversity, core methodological elements reveal that participants are considered knowledgeable, reflexive individuals who can better articulate their complex life journeys when painting and drawing their bodies and social circumstances. The decolonization of health research occurs when these unlikely protagonists tell their stories producing counter-hegemonic discourses to exclusionary capitalist, patriarchal and colonialist rationalities. We call this methodology body-map storytelling.
Key words: body map; qualitative methodology; qualitative health research; arts-based research; visual methods; transformative methods; postcolonial; marginalized; stigmatized participants
Table of Contents
1. Introduction
2. Challenging the Colonization of Health Research
3. Body Mapping: Historical Roots
4. Methodology
4.1 Creating research questions
4.2 Identifying and selecting relevant studies
4.3 Charting and analyzing data
5. Findings
5.1 Contextual information: Interdisciplinary, international and increasingly utilized as a methodology
5.2 Content: An emergent methodology
6. Discussion
6.1 The BMST methodology in the health sciences
6.2 Methodological features
6.3 Theoretical orientations
6.4 Decolonizing health research
7. Final Remarks
Although some forms of health research have been evolving in order to encompass the complexity of human health as a social, political and economic phenomenon, David NAPIER et al. (2014) argue that the failure to utilize research methodologies that critically examine social structures, hierarchical practices, and cultural understandings is the single greatest barrier we presently face in achieving better health. [1]
We believe body mapping could potentially contribute to the examination of this complexity since previous work has identified it as a valuable approach to studying the intersections of "contextual factors that influence the health and well-being (...)" (GASTALDO, MAGALHÃES, CARRASCO & DAVY, 2012a, p.8) and as an "effective means of depicting social processes and relationships (...) [which has] the capacity to represent symbolically the ways in which interactions with others and cultural meanings are inscribed and performed through the body" (DE JAGER, TEWSON, LUDLOW & BOYDELL, 2016, §29). Thus, we reviewed the literature on body mapping within health research to systematize recent advancements and to contribute to its development from a methodological perspective—i.e., to overcome some of the health research limitations NAPIER et al. (2014) identified. In this article, we show that, to date, the utilization of body maps in health research internationally has been highly attuned to political contexts, physical conditions and people's subjectivities. This sensitivity offers great possibilities for the critical examination of structures, power-mediated and culturally-filtered notions, and practices that shape Western understandings of health. We understand such critical scrutiny as one essential way of decolonizing health research (Section 2 and 3). In addition, we argue that body mapping, despite being predominantly presented as a data generation method in our literature review (Section 4), is no longer a method but rather a methodology given its recent utilization within health research (Sections 5 and 6). [2]
Therefore, exploring the possibilities and limitations of body mapping as a research methodology within health research is our attempt to contribute to decolonizing the health sciences and expanding academic horizons. As BERMÚDEZ, MURUTHI and JORDAN (2016) underscore, we aim to scrutinize the legacy of Western ideologies within health research. However, while we offer decentering alternatives, we also identify theoretically and practically underdeveloped methodological elements. [3]
2. Challenging the Colonization of Health Research
Postcolonial scholars have often denounced the false universalism of Western scientific endeavors, emphasizing the epistemological assumption that all forms of knowledge are incomplete, and affirming that a lack of cognitive justice1) is at the source of many forms of inequities in a globalized world (SANTOS, ARAÚJO & BAUMGARTEN, 2016). From this perspective, science could be conceived as a project of capitalist, colonial, and patriarchal domination (ibid.). [4]
As a form of critique to Eurocentric and imperialist academic practices, scholarship on decolonization has emphasized a new standpoint from which different narratives around bodies and minds can emerge. Linda Tuhiwai SMITH's (2012) seminal work proposes that the assumptions underlying Western research are based on an authoritative representation of the Other, wherein the researcher's gaze is constitutive of universal truth. Mindful of these colonization effects, we believe that as scientists who belong to the global North and South concomitantly, we should make visible alternative and counter-hegemonic perspectives by focusing on silenced health experiences. As SANTOS explains, "the sociology of absences consists of an inquiry that aims to explain that what does not exist is, in fact, actively produced as non-existent, that is, as a non-credible alternative to what exists" (2004, p.238). [5]
We are cognizant that body maps have been used across several research and intervention realms, from sexuality education to human-computer interaction and design (DE JAGER et al., 2016; HELMER, SENIOR, DAVISON & VODIC, 2015; NÚÑEZ-PACHECO & LOKE, 2016). Despite outstanding potential for adaptation, we identified that, across the disciplines, body-map projects are intrinsically connected to emancipatory research perspectives, social activism, and alternative media initiatives. However, in the realm of health research, where we have been working for the last two decades (GASTALDO, 2016), there has been a wave of evidence-based discourses and approaches to knowledge production undermining qualitative and arts-based evidence (EAKIN, 2016; GASTALDO, 2016). In this context, we choose to challenge the higher status of one form of knowledge to move beyond "knowledge as regulation" and decolonize methodologies (SANTOS, 2007a, p.410). [6]
To this end, two principles justify our intent. Firstly, while we understand that health research must remain committed to the highest scientific standards, we argue that science as a "single global model of rationality" (SANTOS, 2007b, p.16) must be thoroughly examined in order to achieve cognitive justice. Thus, understanding that the epistemological standpoint from which we investigate focuses not only on what happens to our bodies—which is generally the focus of health research—but also aims to uncover how this knowledge has been used to separate (through power dynamics and oppressive practices) or to bind us together (through alliances and emancipatory processes). Knowing as a means of solidarity is therefore a theoretical lens that can help to decolonize health research (SANTOS, 2007a). [7]
Secondly, despite the increase of qualitative schools of inquiry, a pervasive shortcoming of contemporary mainstream health research is the dominance of verbal methods that sometimes fail to consider the perceptual mediation that may play a role in data generation and analysis (LINELL, 2009). Commonly, in qualitative health research, whatever people say is taken as real, given the epistemological dominance of positivist approaches to research, which ignore the possibility of polyvocality. As the anthropological and linguistic traditions assert, polyvocality generally means many voices, but in its deeper sense, it articulates the power dynamics that organize discourses (ibid.). As PITHOUSE-MORGAN and colleagues (2014) state, there is an urgent need for pluralism of stories, and, to which we would add multiple meanings attributed to a situation experienced by different social actors. [8]
The potential of body mapping to decolonize knowledge production in the health sciences relates to its ability to create a greater range of voices through research, but also to "engage participants as co-producers of knowledge," and disrupt "mechanisms that maintain hierarchies of exclusion" (PARKER, HOLLAND, DENNISON, SMITH & JACKSON, 2017, p.2). Over the past several years, despite some variations in its application, researchers utilizing body mapping went beyond simply using it as method for data generation to address its underpinnings as a qualitative approach, including theory-design links, participants' roles, visual and narrative elements for analysis, etc. (CARTER & LITTLE, 2007). For this reason, in its current level of development and utilization, we argue that body mapping is a research methodology with strong links to decolonization of knowledge production. [9]
3. Body Mapping: Historical Roots
Even though mapping the body and the environment where one works or lives has long been used for data collection, the research activity (the life-size bodily depiction of a person) evolved from social and health sciences' multiple adaptations of advocacy and therapeutic uses. This was undertaken mainly in African countries in the early 2000s (DE JAGER et al., 2016; ORCHARD, 2017; SOLOMON, 2007; WIENAND, 2006). Body mapping has been generally defined as "the process of creating body-maps using drawing, painting, or other art-based techniques to visually represent aspects of people's lives, their bodies and the world they live in" (GASTALDO et al., 2012a, p.5; see Figure 1 for an example).
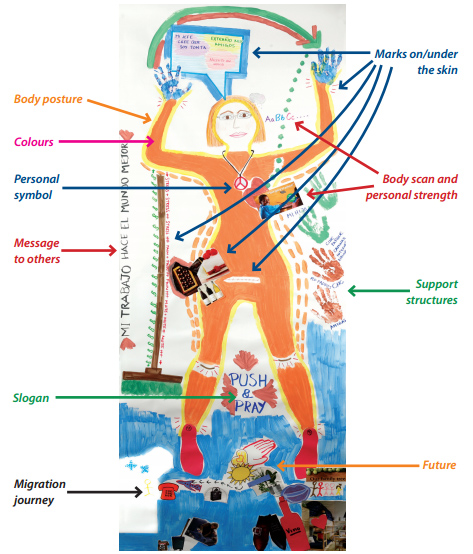
Figure 1: Example of a body map (GASTALDO et al., 2012a, p.16, reprinted with permission) [10]
In the 1990s, the AIDS and Society Research Unit (ASRU) in South Africa launched the Memory Box project to help HIV-positive parents and their children to prepare for death, decorating handcraft boxes in which usually mothers would place sentimental or historical objects for their children. This project was inspired by the Memory Work project, started in 1997 in Uganda (WARD, NABWIRE, MAGERO & BIRYETEG, 2006) and narrative therapy principles (WIENAND, 2006). As some participants of the Memory Box workshops started antiretroviral therapy, they wanted to share their stories of living with HIV with a broader audience. At this point, the Life Long Project, developed by ASRU for advocacy between 2001 and 2003, incorporated the artistic and visual representation of the body as a way to create personal stories, as well as to present them to a wider audience (SOLOMON, 2007; WIENAND, 2006). Thus, body-mapping's roots are in multi-purpose, uniting approaches to art and narrative therapy, knowledge production, and advocacy. [11]
Since its origins, body maps have been used in a variety of countries, contexts, and disciplines with different aims (DE JAGER et al., 2016). For instance, in Kenya, they have been used for advocacy and therapy in different projects with marginalized groups, such as people living with HIV or orphans (ART2BE)2). In Japan, body maps were used for an activist exhibition on women's health (TRUST FOR INDIGENOUS CULTURE AND HEALTH, 2015). In education, body maps have been utilized to approach students' rights in Colombia (CHAVES, 2015) and nurses' training in Canada (MAINA, SUTANKAYO, CHORNEY & CAINE, 2014). As a research method, they have been applied to a variety of issues, from undocumented workers' health (GASTALDO, CARRASCO & MAGALHÃES, 2012b) to the experiences of "coming out of the closet"3) (MURASAKI & GALHEIGO, 2016). [12]
In this article we explore how body maps have been utilized in health research, considering what has been done to date and envisioning future developments to advance the decolonization of health research. To that end, we argue that the process of creating body maps (BMs) is named "body mapping" (BM) and often encompasses visual, narrative, and participatory data generation as well as analytic methods. As such, we will adopt the expression "body-map storytelling" (BMST) to describe a methodology that captures these three elements, even though many of the papers reviewed refer to their approach as "method" or "technique," or only partially utilize all three features. [13]
We conducted a critical narrative synthesis of the literature published up to September 2016 to describe how BM has been used in health research. We adapted ARSKEY and O'MALLEY's (2005) scoping review framework taking a critical narrative perspective (CHASE, 2005). Our review involved three steps: 1. creating research questions; 2. identifying and selecting relevant studies; 3. charting and analyzing data. [14]
4.1 Creating research questions
The two main questions that guided the review were: 1. How has BM been utilized in health research? 2. How does BM advance a decolonization agenda in health research? In Table 1, we list the specific questions that were created in an iterative process to address the study goals, theoretical framework, and empirical findings. They are:
|
Regarding utilization: |
|
In which countries and within which disciplines has BM been used? |
|
How has BM been labeled? |
|
What are BM's shared features? |
|
How are they utilized in data generation? |
|
How is data analysis conducted? |
|
Which insights have researchers shared about the BM? |
|
Regarding decolonization: |
|
What are the epistemological stances adopted by researchers? |
|
What are the health issues explored through BM? |
|
Which groups are involved in research when using BM? How do they participate? |
Table 1: Guiding questions for data analysis [15]
4.2 Identifying and selecting relevant studies
A purposeful sampling strategy was applied to select health research publications in which BM was used as a method for data generation (SURI, 2011). Given the interdisciplinary nature and blurred boundaries of "health" (and, subsequently, "health research") as a concept, we decided to use HUBER and colleagues' approach. These authors propose "a generally agreed direction in which to look," rather than a fixed definition of health, and suggest understanding health as "the ability to adapt and to self-manage" (2011, p.236). Then, we adopted the World Health Organization (WHO) definition of health research, considering those studies that produce "knowledge that can be used to promote, restore, and or maintain the health status" (WHO, 2017, §2) of individuals and populations. Therefore, we included health research publications that used BMs (life-size body representation of a person) as a form of visual and oral data generation and excluded those that did not approach health issues and/or social determinants of health; or used BM as a therapeutic intervention or pain assessment tool. [16]
We employed variations of the terms "health," "well-being," "research," and "body mapping" in Portuguese, Spanish, English, and French to retrieve potentially relevant materials. Eleven electronic databases were selected: Scopus, WOK, Embase, CINAHL, African Journal Archive, African Knowledge Project, African Index Medicus, Dialnet, Lilacs, Ibecs, and Scielo. The rationale to choose these databases was two-fold: they index materials in the aforementioned languages and they cover diverse geographical locations such as Europe, North and South America or Africa. We also used Google Scholar to review non-indexed material in order to expand the search. [17]
The search in the databases resulted in 296 articles and Google Scholar generated 1,102 entries (Figure 2). We eliminated the duplicates from the different databases, keeping 216 articles to screen. From Google Scholar entries, we selected 83 research publications (e.g., scientific articles, reports, monographs). After eliminating the duplicates, we retained 293 documents to screen. After applying the described inclusion and exclusion criteria, 41 articles remained. [18]
Full texts were retrieved and read by at least two team members to decide if they should be included according to the criteria described above. We encountered a wide variety of approaches to BM as a research tool, as well as reporting styles. Much discussion among team members was required when applying the criteria to specific articles since the boundaries between health and social science research are unclear, or the use of BM as a research technique was not described. If two team members disagreed on whether to include or exclude an article, a third member would contribute to the discussion until agreement was reached. Examples of articles excluded were those employing BM as an educational tool for health care professionals (MAINA et al., 2014), as a coping strategy (NÖSTLINGER, LOOS & VERHOEST, 2015), variations of the BMs which incorporated a pre-established silhouette (LUDLOW, 2014) or uses of BM in non-health research (CHAVES, 2015). Eventually, after this second screening, we retained 23 articles. [19]
The last step was to conduct a review of the reference lists of the selected articles. We identified relevant publications that were not identified during the original search because they were either not yet published or indexed in the databases (e.g., ROSS-QUIROGA, 2013), or were not available online (e.g., GASTALDO, MAGALHÃES & CARRASCO, 2013). This outreach led to the addition of four more documents: one book chapter and three research reports. In total, 27 texts were included for the analysis (see the Appendix).
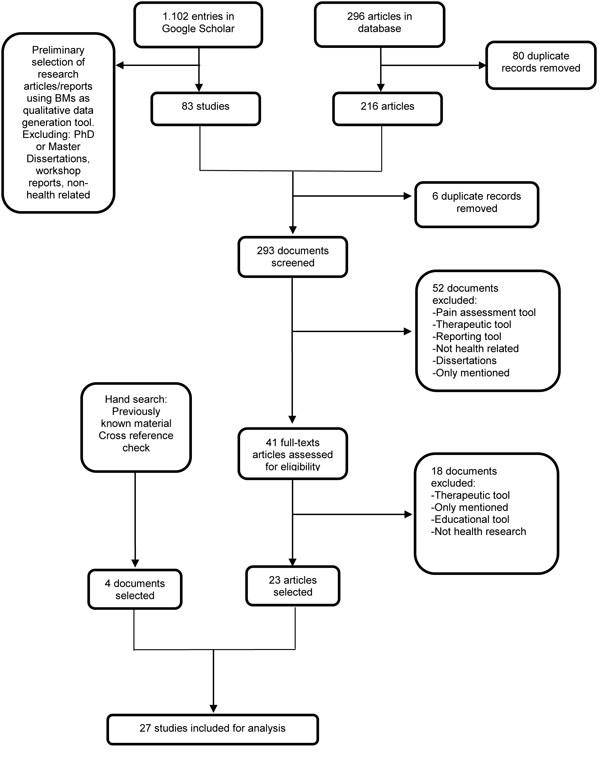
Figure 2: Document search and selection process [20]
4.3 Charting and analyzing data
We analyzed data in terms of the questions included in Table 1 following a critical narrative synthesis approach. First, we read and summarized each article and charted the information as to context, content, and methodological and theoretical considerations on how BM was used in each study (e.g., Was it understood as a method or methodology? Was it used alone or with other tools? What are the study's strengths and limitations?). [21]
We described the distribution and nature of the studies (date, journal, title, authors, authors' countries of affiliation, country of the study, population group, and health topic). This contextual information provides part of the social and academic circumstances that enable or constrain BM project development in health research (CHASE, 2005). [22]
With the support of ATLAS.ti. software, we described each paper's research questions/aims, methodology, main findings, and knowledge translation strategies. Using a critical narrative mode of synthesis, we tried to capture how authors made sense of BM in health research. We re-read the materials coding how BM was used in each of the 27 texts. Next, we searched for similarities and differences across the texts by moving back and forth iteratively through the coded data, and by team discussion that continued until consistency and distillation was achieved. During the analysis, we tried to retain the authors' voices by staying close to their original expressions and denominations. We use an "authoritative voice" to report the findings, speaking "differently from, but not disrespectfully of" authors' voices (CHASE, 2005, p.664). [23]
4.3.3 Methodological and theoretical considerations
We reflected on and recorded how BM was conceived, developed, and applied in each study and how it was described across publications (e.g. theories guiding studies; individual or group sessions). We used this exercise to ensure rigor during the data analysis and to gain an understanding of how BM can contribute to the decolonization of health research. [24]
5.1 Contextual information: Interdisciplinary, international and increasingly utilized as a methodology
Most documents analyzed in this review (85%) have been published in the last six years (see Figure 3).
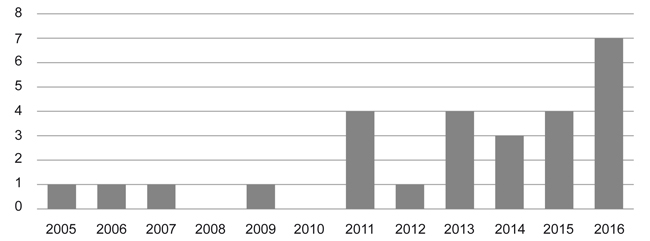
Figure 3: Graph of number of articles published per year [25]
Researchers' institutional affiliations were based in Canada (26%), South Africa (18%) and Australia (11%). Remaining articles correspond to researchers from Brazil (7%), Chile (7%), United Kingdom (4%), Bolivia (4%), and from international collaborations: USA, Canada and Spain (4%), Canada and Brazil (4%), South Africa and United Kingdom (4%), South Africa and Colombia (4%), USA and United Kingdom (4%). [26]
The studies were conducted primarily in South Africa (30%) and Canada (22%), followed by Australia (11%), Brazil (7%), Chile (7%), USA (7%), Bolivia (4%) and the Philippines (4%); one study was located in three different countries (Mexico, Spain and USA). Health topics studied were social determinants of health (44%), HIV (26%), sexual health (18%), pain (4%), health literacy (4%) and others (4%). More than half of participants were adults (54%). Other participants were youth (23%), youth and young adults (8%), young adults (8%) and children (7%). Although generally used with vulnerable groups, we note that BM was performed with able-bodied persons. Seniors and people living with disabilities were absent from the studies. [27]
Although the reporting languages are English, Portuguese, and Spanish (no study in French was found), in many projects the languages used in the research process were participants' mother tongues, like IsiZulu (VAN DE RIET, HOUGH & BEV, 2005), Ilonggo (MITCHELL, 2006), Spanish or Portuguese (GASTALDO et al., 2012a), or Khmer (LEE et al., 2016). [28]
Researchers have varying disciplinary backgrounds and academic/work contexts, including anthropology, development studies, English studies, geography, indigenous health, nursing, occupational therapy and science, physiotherapy, psychology, political science, public health, and sociology. The interdisciplinary scope of BM in health research is notable. The terminology adopted by these authors to name BM is listed in Table 2.
|
English |
Portuguese |
Spanish |
|
Body maps Body mapping Body-map storytelling Body-mapped story Body-map drawing |
Mapas corporais Mapeamento corporal Mapas corporais narrados Narrativa de mapas corporais |
Mapas corporales Mapeo corporal Mapas de los cuerpos Mapa corporal
|
Table 2: Names utilized to describe the methodology [29]
5.2 Content: An emergent methodology
Beyond the increase in publication rates over the last six years, three key narratives identified support the argument that BMST is an emergent methodology. [30]
5.2.1 Common ground: BMs are used to tell stories of marginalized people
BM is used in health research to approach the health and well-being experiences of disempowered people in global societies. Some of these disenfranchised people with whom researchers work are: indigenous and non-indigenous youth (CHENHALL, DAVISON, FITZ, PEARSE & SENIOR, 2013; HELMER et al., 2015; SENIOR, HELMER, CHENHALL & BURBANK, 2014); children living in poverty (MITCHELL, 2006) or living with HIV (VAN DE RIET et al., 2005); women and men living with HIV (HORNE, 2011; MacGREGOR, 2009; MacGREGOR & MILLS, 2011; ORCHARD, SMITH, MICHELOW, SALTERS & HOGG, 2014); sex workers and transgender persons (ROSS-QUIROGA, 2013); women who have suffered forced sterilization (STEVENS & LE ROUX, 2011); people self-identified as part of lesbian, gay, bisexual, transgender, queer (LGBTQ) communities (DILL, VEAREY, OLIVEIRA & CASTILLO, 2016; MURASAKI & GALHEIGO, 2016; OLIVEIRA, MEYERS & VEAREY, 2016); low status workers (SHUMKA & BENOIT, 2007); and refugees and migrants (DAVY, MAGALHÃES, MANDICH & GALHEIGO, 2014; GASTALDO et al., 2012b, 2013; OLIVEIRA et al., 2016). [31]
Researchers approach health from broad perspectives in which participants' health and well-being are narrated from inextricable social and personal perspectives. For instance, SENIOR et al. (2014) engage in a discussion about young people's risky sexual behavior in Australia, highlighting the key role of youths' perceptions of vulnerability to sexually transmitted infections as well as the social context shaping these conceptions. GASTALDO et al. (2012b) studied undocumented migrant workers' health experiences in Toronto by contextualizing their experiences within larger political and economic processes embedded in globalization. Similarly, SMIT et al. (2016) tied non-communicable diseases among residents from a low income area of Cape Town to the negative impact of the built environment, which has been historically and socially shaped. [32]
Within these studies of politically contextualized health experiences the researchers present BM as a suitable tool for data generation by putting forward four main arguments: 1. BMs allow researchers to generate contextualized and multilayered information about life trajectories and health experiences (GUBRIUM, FIDDIAN-GREEN, JERNIGAN & KRAUSE, 2016; MacGREGOR, 2009; OLIVEIRA et al., 2016; SMIT et al., 2016); 2. create spaces for participants to convey their stories in their own terms, actively participating in the data generation process, choosing what information they consider relevant or are willing to share (DAVY et al., 2014; GASTALDO et al., 2013; MURASAKI & GALHEIGO, 2016; STEVENS & LE ROUX, 2011); 3. do the combinations of visual, textual and oral information whose complementary nature facilitate understanding of participants' complex stories (GASTALDO et al., 2013; HORNE, 2011; MITCHELL, 2006; VAN DE RIET et al., 2005); 4. although less frequently cited, BM is presented as a catalyst for awareness-raising projects (DONELLE, HALL & BENBOW, 2015; LEE et al., 2016; OLIVEIRA et al., 2016). [33]
The most frequently used concepts of BM are those provided by CORNWALL (1992), SOLOMON (2007), and GASTALDO et al. (2012a) (see Table 3). Some researchers use a combination of these concepts as rationale or to introduce BM.
|
CORNWALL (1992) |
"Body-maps can be used for gaining access to people's perceptions of their bodies and to the explanatory models which people bring into encounters with health care workers. Representing this information visually can help to clarify ambiguities and provides a rapid shared reference point. By using people's own representations of their bodies as a starting point from which to explore particular medical issues, body-mapping can facilitate a less directive interviewing style than would otherwise be possible. People's own classifications and visual descriptions can be used as a basis for probing" (pp.69-70). |
|
SOLOMON (2007) |
"When we make a body-map, we outline the shape of the human body as a starting point so that we can make life-size pictures of ourselves. Our body-maps include everything that we feel is most important about ourselves. (...) Body-mapping uses drawing and painting exercises, visualization (using your imagination), talking in groups, sharing, and quiet times for just thinking and reflecting on what is happening. The body-mapping process often includes a lot of singing, dancing and acting as well" (p.2). "Body-mapping can help each person to understand and explore his or her own life, but it can also reach out to other people in social and political ways" (p.3). |
|
GASTALDO, et al. (2012a) |
"... the process of creating body-maps using drawing, painting or other art-based techniques to visually represent aspects of people's lives, their bodies and the world they live in" (p.5). |
Table 3: Most frequently used BMs/BM concepts [34]
In order to tell participants' stories, BM generally combines drawing with other data generation tools, mostly to aggregate a strong narrative component to the creation of the maps. Both traditional and more innovative qualitative techniques are used alongside BMs, generally aiming to deepen or complement participants' narratives (GASTALDO et al., 2012b; QUIJANO & VIEIRA, 2016). Well-established tools used are: individual interviews (GASTALDO et al., 2012b; ORCHARD et al., 2014) in which, sometimes, the researcher and participant create a testimonio4) and a legend to enhance the understanding of the visual elements of the BMs (GASTALDO et al., 2012b); individual interviews and focus groups or group interviews (ROSS-QUIROGA, 2013; SENIOR et al., 2014; SILVA & MÉNDEZ, 2013); focus groups and individual interviews in combination with other activities (RAMSURAN & LURWENGU, 2008; ROSS-QUIROGA, 2013; VAN DE RIET et al., 2005); and interviews and participant observation (QUIJANO & VIEIRA, 2016). More innovative alternatives such as writing and poetry workshops (DILL et al., 2016; OLIVEIRA et al., 2016), popular theater and interpretative art-making (LEE et al., 2016) were also employed. When used alone, the creation of BMs is accompanied by some kind of conversation which is not described as a separate data generation tool (DAVY et al., 2014). Also, others have described how participants and facilitators talked and shared experiences during the BM as part of the data generation process (STEVENS & LE ROUX, 2011; SWEET & ESCALANTE, 2015). Our interpretation of these varied techniques and combinations is that these scholars are using BMST as a methodology (no longer a single method) that comprises participatory, narrative, and arts-based components. [35]
When BM is considered a method, researchers name their study methodologies as qualitative inquiry according to a particular theory or discipline (e.g., phenomenology or anthropological thought), generic qualitative research (MacGREGOR & MILLS, 2011; MURASAKI & GALHEIGO, 2016), qualitative research using visual methods (DILL et al., 2016; GASTALDO et al., 2013), qualitative case study (DONELLE et al., 2015), and participatory methodologies, such as mixed-method action research (ROSS-QUIROGA, 2013) and community-based participatory research (LEE et al., 2016). [36]
The studies using BM are all guided by either interpretivist or critical onto-epistemological perspectives (ESPINOZA-TAPIA & SEGOVIA, 2015; SILVA & MÉNDEZ, 2013). In some cases, authors explicitly report these onto-epistemological tenets and articulate them consistently in the methodology (LEE et al., 2016; OLIVEIRA et al., 2016; ROSS-QUIROGA, 2013; SILVA & MÉNDEZ, 2013). In other cases, these perspectives are embedded in the study and referred to in a particular section (MURASAKI & GALHEIGO, 2016; SMIT et al., 2016). Either way, there is a consistent relationship between the combination of theoretical positions and the methodological development of the study. The more critical the approach, the more innovative the tools combined with BM are, and the more awareness-raising features of BM are highlighted (LEE et al., 2016; OLIVEIRA et al., 2016). [37]
5.2.2 BM in practice: Learning from researchers' experience of generating and analyzing data
When put into practice, the process of BM reveals its purpose and particular forms. BM can be done individually or collectively. An individual BM entails one participant and one researcher working in partnership, guided by the participant's descriptions of visual elements and the researcher's assistance in creating them (e.g., DAVY et al., 2014; MURASAKI & GALHEIGO, 2016; SHUMKA & BENOIT, 2007). This option is frequently chosen to ensure confidentiality (MURASAKI & GALHEIGO, 2016). [38]
Collective BM can be done in three ways. The first alternative is for a group of people to share the space while doing their individual BMs, which can assist with logistics (e.g., tracing another participant's silhouette on the canvas) (MITCHELL, 2006). While participants share a common space, the creation of the BMs, however, is done by each individual with no exchange among participants. The second approach is for the group to actively participate in the creation of each individual's BM. For instance, in the MoVE project study (OLIVEIRA et al., 2016), each participant first produced then explained her or his individual map. While each map corresponded to one individual, the process and final product was co-created; the group members provided feedback on each other's BMs to ensure that the artistic creation accurately conveyed what each participant intended to say. Finally, a collective BM is performed when the group co-creates one body map (CHENHALL et al., 2013; HELMER et al., 2015; ROSS-QUIROGA, 2013), which has been named "collective storytelling process" (HELMER et al., 2015, p.160). One example is reported by CHENHALL et al. (2013), who created hypothetical scenarios to approach sexual health concerns for young people. Researchers presented these scenarios describing some young people's fictional situations and posed questions about what the characters would be experiencing. Participants were encouraged to collaborate in small groups and were instructed to draw and discuss these scenarios using BMs. The group sizes for collective BM range from 2-4 (ibid.; see also SWEET & ESCALANTE, 2015) up to groups of 10 to 20 participants (respectively, SMIT et al., 2016 and CHENHALL et al., 2013). Other studies do not describe how many people were involved in each session of collective body mapping (MITCHELL, 2006; VAN DE RIET et al., 2005). [39]
We have identified three different purposes for creating BMs within the data generation process. Eliciting individual or collective conversations (storytelling) is the most common purpose, as illustrated by CHENHALL et al. (2013) in the aforementioned example. For other authors, creating BMs is useful to condense and convey stories, but also to raise awareness through the research process (ESPINOZA-TAPIA & SEGOVIA, 2015; LEE et al., 2016; SILVA & MÉNDEZ, 2013). For instance, SILVA (2013) describes the BM as a "phase in which all the stories, conversations, lifelines and autobiographies are collected to feed the body-map (...), it is the time when the biographical knots have been opened for the recovery, reflexivity and textual creation" (p.68). Finally, BM is used for secondary analysis (HORNE, 2011) or to trigger further data generation in a new study. Thus, some researchers have created the opportunity for participants to go back to their maps before they were interviewed for a second time (MacGREGOR & MILLS, 2011) or to be used for poetry workshops (DILL et al., 2016; OLIVEIRA et al., 2016). [40]
The combination of data generation tools as well as the purpose and forms of BM show how researchers understand their studies as unfolding processes. In such processes there is not a clear demarcation between data generation methods; rather, data are generated by building from one technique to the next. For example, BM can trigger a group discussion and interviews can work to clarify elements of the map (SENIOR et al., 2014). Or, as we noted, a writing workshop and a BM workshop can be used as data generation techniques, feeding each other in the creation of the final BM, which will later be revisited to generate additional data through a poetry workshop (DILL et al., 2016). These different strategies require varied approaches to verification to remain authentic to participants' views on presentation and representation of the self in the study. [41]
These different forms of BM in practice illustrate the role of facilitators as key to supporting the BM process. While intersubjectivity is a central element mediating BM (GASTALDO et al., 2013), some authors briefly describe facilitators' roles as workshop facilitators (ORCHARD et al., 2014), community experts (GUBRIUM et al., 2016; LEE et al., 2016), research assistants (MITCHELL, 2006) and researchers (CHENHALL et al., 2013). Others explicitly address facilitators' roles and reflexivity (GASTALDO et al., 2012b; MURASAKI & GALHEIGO, 2016; OLIVEIRA et al., 2016; ROSS-QUIROGA, 2013; SWEET & ESCALANTE, 2015). In any case, a trusting relationship between facilitators and participants is reportedly essential to the creation of BMs (CHENHALL et al., 2013; GASTALDO et al., 2013; GUBRIUM et al., 2016; OLIVEIRA et al., 2016; SENIOR et al., 2014). [42]
As in other qualitative methodologies, the description of data analysis processes is frequently either omitted (DILL et al., 2016; HARTMAN, MANDICH, MAGALHÃES & ORCHARD, 2011; HORNE, 2011; MacGREGOR, 2009; ORCHARD et al., 2014; SMIT et al., 2016; STEVENS & LE ROUX, 2011) or minimal (CHENHALL et al. 2013; DILL et al., 2016; OLIVEIRA et al., 2016; ROSS-QUIROGA, 2013). Nevertheless, in their articles, authors frequently take for granted that data generated orally (in interviews, focus groups or group interviews, among others) are included and combined in the analysis. [43]
When data analysis is described, authors focus either on the transcriptions or on the complexity of the BM process. Thus, surprisingly, in some cases, there is a focus on the transcription of the BM meetings or interviews, but no visual data is analyzed (SHUMKA & BENOIT, 2007; VAN DE RIET et al., 2005). Other authors use a more comprehensive analytical approach. This entails an understanding that data generation and data analysis occur simultaneously, and both the process and its products (visual: the maps; narratives: information about the maps; and oral: recorded conversations during the creation of the maps) are valuable data for analysis. Some of the theories or frameworks used to inform such analysis include postcolonial and feminist approaches (GASTALDO et al., 2013), visual data analysis (ROSE, 2006; SWEET & ESCALANTE, 2015) or the notion of intertextuality understood from a critical paradigm (ESPINOZA-TAPIA & SEGOVIA, 2015; SILVA & MÉNDEZ, 2013). [44]
When authors use a comprehensive analytical approach, researchers' reflexivity and participants' involvement in meaning-making are seen as key elements for interpretation, despite varied ways of operationalizing this idea. For instance, according to GASTALDO et al. (2012b, 2013), the first analytical level is the creation of the body map, a time when researcher and participant co-construct meanings (it might or might not include a testimonio and/or a reading key), but a second level of analysis is done exclusively by researchers who conduct inductive and deductive analysis for each individual body map and/or across several body maps. [45]
Other researchers, such as SWEET and ESCALANTE (2015), differentiate a first phase, in which meaning-making is collaboratively performed, and a second phase, in which they use the notions of composition, semiology, and discourse as "code-framing categories" (p.1835) to analyze the BMs. In this case, the interpretation is made based on the location of objects on the map, symbols, and the oral and written narratives. Differently from the two previous strategies, ESPINOZA-TAPIA and SEGOVIA (2015) and SILVA and MÉNDEZ (2013) organize the analytical process in two phases with three dimensions: narrative (oral and written), graphic (maps), and projective (the symbolic products from the previous dimensions). The first phase entails a reorganization of the stories created using the lifeline or autobiographical writing, as well as the body maps. This includes creating a table in which the three dimensions are interrelated (see SILVA, 2013, p.75). In the second phase, researchers examine links between the dimensions and use theory (deductive approach) to refine the analysis and to answer the research question. Finally, key points and conclusions are generated with the participants. These two phases are developed in collaboration with the participants, although the specific steps taken in both studies are not disclosed. [46]
Even though the majority of articles present analysis performed by the researchers (DAVY et al., 2014; DONELLE et al., 2015; GASTALDO et al., 2012b, 2013; MITCHELL, 2006; MURASAKI & GALHEIGO, 2016), some researchers collaborate with participants to analyze data. For example, ROSS-QUIROGA (2013) describes a horizontal co-analysis in which participants provide interpretations, while GUBRIUM et al. (2016) state that co-analysis is of fundamental importance: it is the participant's role to generate and interpret her or his BM and the researcher's role to identify common themes. LEE et al. (2016) used a facilitation team that moderated democratic discussions in small groups where analysis and interpretation occurred collaboratively. The summaries of the discussions of each small group were examined in a larger group context. When a decision needed to be made, the full group voted. Nevertheless, in these cases a limited description of the analytic process is offered. [47]
Researchers identify several challenges when using BMST in health research. Logistics, including limited time and space, might interfere with participants' and researchers' ability to create BMs (HARTMAN et al., 2011). Also, drawing skills pose a challenge. It has been argued that special attention should be paid to participants' concerns about their artistic abilities and researchers should emphasize that artistic expression is the means and not the end of the process (DAVY et al., 2014; HARTMAN et al., 2011). Ethical challenges have also been mentioned, especially regarding participants' engagement and confidentiality (CHENHALL et al., 2013; MITCHELL, 2006; VAN DE RIET et al., 2005), as well as maintaining anonymity while graphically telling detailed stories through BMs (GASTALDO et al., 2012b; GUBRIUM et al., 2016; OLIVEIRA et al., 2016), particularly when the map is later used for knowledge translation or publications. Participants who want to remain anonymous may have difficulties engaging with a visual storytelling approach to research, especially because attending several sessions may be noticeable to community or family members (e.g., GASTALDO et al., 2012b, had to create several measures to facilitate participation). In terms of confidentiality, stigmatized conditions or circumstances, such as HIV/AIDS, homosexuality, lack of migratory status or citizenship can expose participants to unintended disclosure and even deportation. [48]
Lastly, some authors reflect on the complexities of data analysis. A particular concern has been how to move from a descriptive level to an interpretive level utilizing both visual and oral data (GASTALDO et al., 2012b; VAN DE RIET et al., 2005). [49]
Some advantages of BM identified by researchers are that it generates multilayered, contextualized data, revealing complexities, richness, wholeness, and unique insights (GASTALDO et al., 2013; MacGREGOR, 2009; MITCHELL, 2006; OLIVEIRA et al., 2016; ORCHARD et al., 2014; ROSS-QUIROGA, 2013). For example, ROSS-QUIROGA (2013) states that BMs create visual data of women's experiences of visible and invisible violence within a specific context. [50]
Some researchers reflect upon the elicitation process achieved through drawing with participants. Drawing allows participants to distance themselves from their experiences, which may prevent them from being overwhelmed by memories, as well as contribute to reflection, organization of past experiences, and deeper understanding (HARTMAN et al., 2011; HORNE, 2011). Investigators also report that BM contributes to participants' empowerment, ownership of their lives, and learning about different topics (DILL et al., 2016; HARTMAN et al., 2011; MITCHELL, 2006; OLIVEIRA et al., 2016; STEVENS & LE ROUX, 2011). Others go further to suggest BMs as an advocacy tool, organizing exhibitions and inviting public dialogue (DILL et al., 2016; GASTALDO et al., 2012b; GUBRIUM et al., 2016; MITCHELL, 2006; OLIVEIRA et al., 2016), and state that BM has the potential to question what is valid knowledge, serving as "transformative evidence" in health research (GUBRIUM et al., 2016, p.621). Similarly, SILVA (2013) proposes that BM opens new methodological connections to study biographical processes, causing an interpellation of existing methods. [51]
These considerations reveal the recent development of BMST as a visual, narrative, and participatory methodology, despite uneven utilization of these three components by many researchers. [52]
6.1 The BMST methodology in the health sciences
This article documents the emergence of BMST as a health research methodology, even though there are several nomenclatures utilized to describe it in different languages. We propose to move away from the generic term "body map" and to add the term "storytelling" to differentiate the methodology from the other uses of BM as a method to map the body within a physical space or display illness signs and symptoms. As we see it, BMST is a methodology that brings together the visual representation of the person's body in natural size and narratives about the symbols selected to explain how the person came to be what she or he currently is, which are co-produced in a participatory manner between the research participant(s) and the researcher(s). Such richness of data, however, presents certain challenges. Perhaps in the health sciences, the difficulty of concurrently analyzing visual and verbal data has made some researchers emphasize oral over visual data, given that interviews are the most familiar method for data "collection" and analysis. [53]
Despite its diversity, we have identified some core methodological elements of BMST, such as the shared axiological commitment of engaging participants as knowledgeable, reflexive individuals who can better articulate their complex life journeys if tools, such as drawing and painting their bodies and social circumstances, are used to promote expression. Within this process, a narrative component is clearly present when using BM in health research. However, this has been operationalized differently by researchers. For example, GASTALDO et al. (2012b) name an outcome of the narrative process testimonio. Other researchers named or used other data generation methods (e.g., group discussion, interview, writing and poetry workshops, etc.) to articulate this narrative feature (DILL et al., 2016; ORCHARD et al., 2014; OLIVEIRA et al., 2016; ROSS-QUIROGA, 2013; SENIOR et al., 2014; SILVA & MÉNDEZ, 2013). While BMST originates in the global South, it is utilized by both Northern and Southern researchers. Interestingly, this methodology is almost in a 50/50 split, utilized by some in the native language of the participants irrespective of the geographical location of the study, which reveals elements of solidarity with participants (i.e., promoting their full potential of expression) and commitment to critical methodological inquiry. Another feature is the utilization of BMST by those in the humanities, social sciences, and health sciences to study health issues with a shared agenda for social transformation, favoring topics related to the social determinants of health of marginalized groups. [54]
Our review also shows considerable variation in the theoretical foundations and strategies for data generation and analysis. The onto-epistemological foundations of the methodology draw on both critical and interpretivist research paradigms, similar to what LINCOLN and GUBA (2013) have named "interpretive critical inquiry" (p.89), which aims to achieve an in-depth understanding of lived experience, yet acknowledges social conflict and is critical of the potential marginalization that research may cause. BMST associates narrative and symbolic ways to elicit understanding for a critical, emancipatory agenda that makes visible social actors who have very limited social capital to influence politicians, policy-makers, or health care managers, and are equally unknown to most dominant groups in society (e.g., women victim of violence, HIV-positive mothers, LGBTQ people, and undocumented workers, among others). [55]
6.4 Decolonizing health research
BMST can support the decolonization of health research as it creates visibility for marginalized social actors, opportunities to tell stories of unlikely protagonists in the social sphere, and can potentially produce counter-hegemonic discourses to exclusionary capitalist, patriarchal, and colonialist rationalities. However, the dominance of positivism in the health sciences also means it will be challenged, like other forms of qualitative research, as non-scientific (i.e., it may be labeled as "just stories," as we have been told before). Articulating ideas of cognitive justice, avoiding epistemicide5), and transforming "stories and drawings" into evidence to support public policy development or improve health care still defy the imagination of many positivist health researchers globally (SANTOS, 2004, 2007a). As qualitative methodologies remain at the bottom of the hierarchy of evidence (EAKIN, 2016), BMST should be considered a methodology for resistance and transformation in the health sciences. [56]
In order to help expanding the academic horizon, we believe health researchers who utilize BMST should work towards greater methodological clarity and consistency, not decreasing their diversity of approaches, but rather theorizing and describing strategies utilized to support other researchers' methodological choices. Unfortunately, most researchers do not take advantage of the full potential of BMs for knowledge production and mobilization in community, institutional, and political settings. The creation of visual stories, poetry, exhibitions, posters for community use, as well as scientific presentations and articles reveal BMST's potential for advocacy both at the margins and at the core. [57]
In this period of multiple and sometimes divergent uses of this methodology, the lines researchers have been drawing may seem like blurred methodological attempts, but the accounts they have created with participants depict clear pictures of alternative understandings of health phenomena, based on elicitation, participation, and co-production of knowledge. In doing so, different forms of knowing are apprehended through blurred lines drawn together, articulated through a combination of multisensorial, political, cognitive, emotional, and reflexive means, which yields for a literal and metaphorical bricolage approach to storytelling (KINCHELOE, 2001; SANTOS, 2007a). [58]
This review reveals the broad scope of BMST for health research. Despite remarkable growth, BMST remains mostly under-theorized, and is hence at risk of being misunderstood and misused. There is, however, great opportunity for future development, whether we further investigate its visceral nature, as suggested by SWEET and ESCALANTE (2015), or we recognize that BMST encompasses a narrative that disputes traditional views of space and time, as well as dichotomies such as health and sickness, public and private, individual and social. Further, while engaging people in collective reflexive creation, BMST might serve as a tool to foster change through an exercise of praxis, as FREIRE (2005 [2000]), suggests:
"For apart from inquiry, apart from the praxis, individuals cannot be truly human. Knowledge emerges only through invention and re-invention, through the restless, impatient, continuing, hopeful inquiry human beings pursue in the world, with the world, and with each other" (p.72). [59]
The undeniable acceptance and application of BMST within some forms of contemporary health research makes us confident that it has a promising role to play in the global research landscape, leading us to a clearer and sharper perspective about diverse and inclusive realities. [60]
Click here to download the PDF file.
Natalia RIVAS-QUARNETI received doctoral fellowships from Barrié de la Maza Foundation (2014) and from University of A Coruna (2016) which supported the development of this article. The authors acknowledge the contribution of Dr. Joan EAKIN, Dr. Martyna JANJUA, and Mr. David GEROW for the language review and the anonymous reviewers for their constructive criticisms.
1) Cognitive justice means the acknowledgment of a plurality of ways of knowing and their equal value. These different knowledges should dialogue in a horizontal relationship to challenge hegemonic hierarchies that underpin injustices. Cognitive justice is a prerequisite for social justice (SANTOS et al., 2016). <back>
2) See Sophie KELLIHER's (Art2Be) personal reflection on a body-mapping exhibition in Nairobi http://www.gizkenyahealth.com/blog/body-mapping-exhibition-in-nairobi-attracts-crowds/ [Accessed: November 28, 2017] or the "Body Mapping Projects" website https://kindevelopment.wordpress.com/international-projects/ [Accessed: November 28, 2017] as examples. <back>
3) All translations from Portuguese and Spanish to English in this article are ours. <back>
4) Testimonio is a Spanish word used to describe a very personal and meaningful first person narrative about a participant's life event. <back>
5) According to SANTOS (2015, pp.152-153), "the epistemological privilege that modern science grants to itself is thus the result of the destruction of all alternative knowledges that could eventually question such privilege. It is, in other words, a product of what I called in a previous chapter epistemicide. The destruction of knowledge is not an epistemological artifact without consequences. It involves the destruction of the social practices and the disqualification of the social agents that operate according to such knowledges." <back>
Arskey, Hilary & O'Malley, Lisa (2005). Scoping studies: Towards a methodological framework. Scoping Studies: Towards a Methodological Framework, 8(1), 19-32.
Bermúdez, María; Muruthi, Bertranna & Jordan, Lorien (2016). Decolonizing research methods for family science: Creating space at the center. Journal of Family Theory & Review, 8(2), 192-206.
Carter, Stacy M. & Little, Miles (2007). Justifying knowledge, justifying method, taking action: Epistemologies, methodologies, and methods in qualitative research. Qualitative Health Research, 17(10), 1316-1328.
Chase, Susan (2005). Narrative inquiry. Multiple lenses, approaches, voices. In Norman K. Denzin & Yvonna. S. Lincoln (Eds.), The Sage handbook of qualitative research (3rd ed., pp.651-679). CA, USA: Sage.
Chaves, Omar (2015). Territorio y derechos. Cartografías corporales en la investigación sobre territorio en los contextos escolares. In Jorge Palacio (Ed.), Cuerpo y educación. Variaciones en torno a un mismo tema (pp.1-172). Bogotá: Instituto para la Investigación Educativa y el Desarrollo Pedagógico, IDEP, http://biblioteca.clacso.edu.ar/Colombia/idep/20160129125118/CuerpoyEducacion.pdf#page=119 [Accessed: August 25, 2016]
Chenhall, Richard; Davison, Belinda; Fitz, Joseph; Pearse, Tiffanie & Senior, Kate (2013). Engaging youth in sexual health research: Refining a "youth friendly" method in the Northern Territory, Australia. Visual Anthropology Review, 29(2), 123-132.
Cornwall, Andrea (1992). Body mapping in RRA/PRA, RRA notes. In Alice Welbourn (Ed.), RRA Notes 16, Special issue on applications for fealth (pp. 69-76). London: International Institute for Environment and Development.
Davy, Charity; Magalhães, Lilian; Mandich, Angela & Galheigo, Sandra (2014). Aspects of the resilience and settlement of refugee youth: A narrative study using body maps. Cadernos de Terapia Ocupacional, 22(2), 231-241, https://doi.org/10.4322/cto.2014.045 [Accessed: August 19, 2016].
de Jager, Adèle; Tewson, Anna; Ludlow, Bryn & Boydell, Katherine (2016). Embodied ways of storying the self: A systematic review of body-mapping. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 17(2), Art. 22, http://dx.doi.org/10.17169/fqs-17.2.2526 [Accessed: August 25, 2016].
Dill, LeConté J.; Vearey, Jo; Oliveira, Elsa & Castillo, Gabriela M. (2016). "Son of the soil ... daughters of the land": Poetry writing as a strategy of citizen-making for lesbian, gay, and bisexual migrants and asylum seekers in Johannesburg. Agenda, 30(1), 85-95.
Donelle, Lorie; Hall, Jodi & Benbow, Sarah (2015). A case study of the health literacy of a criminalized woman. International Journal of Health Promotion and Education, 53(4), 192-203.
Eakin, Joan M. (2016). Educating critical qualitative health researchers in the land of the randomized controlled trial. Qualitative Inquiry, 22(2), 107-118.
Espinoza-Tapia, Ricardo & Segovia, Jimena S. (2015). Emociones, corporeidad y socialización de género en la subjetivación de la masculinidad de jóvenes chilenos: Una aproximación intertextual desde el modelo de mapas corporales. Salud & Sociedad, 5(3), 300-317, http://www.redalyc.org/articulo.oa?id=439742476005 [Accessed: August 25, 2016].
Freire, Paulo (2005 [2000]). Pedagogy of the oppressed: 30th anniversary edition. New York: Continuum.
Gastaldo, Denise (2016). Re: An open letter to The BMJ editors on qualitative research. Rapid responses. The BMJ, 352, i563, http://www.bmj.com/content/352/bmj.i563/rr-21 [Accessed: August 18, 2017]
Gastaldo, Denise; Carrasco, Christine & Magalhães, Lilian (2012b). Entangled in a web of exploitation and solidarity: Latin American undocumented workers in the Greater Toronto Area, http://www.migrationhealth.ca/undocumented-workers-ontario/summary-findings [Accessed: August 15, 2016].
Gastaldo, Denise; Magalhães, Lilian & Carrasco, Christine (2013). Mapas corporais narrados: um método para documentar trajetórias de saúde, resiliência, adoecimiento e sofrimento. In Alex B. Fraga, Yara M. de Carvalho & Ivan M. Gomes (Eds.), As práticas corporais no campo da saúde (pp.83-100). São Paulo: Editora Hucitec.
Gastaldo, Denise; Magalhães, Lilian; Carrasco, Christine & Davy, Charity (2012a). Body-map storytelling as research: Methodological considerations for telling the stories of undocumented workers through body mapping, http://www.migrationhealth.ca/undocumented-workers-ontario/body-mapping [Accessed: August 15, 2016].
Gubrium, Aline C.; Fiddian-Green, Alice; Jernigan, Kasey & Krause, Elizabeth L. (2016). Bodies as evidence: Mapping new terrain for teen pregnancy and parenting. Global Public Health, 11(5-6), 618-635.
Hartman, Laura R.; Mandich, Angela; Magalhães, Lilian & Orchard, Treena (2011). How do we "see" occupations? An examination of visual research methodologies in the study of human occupation. Journal of Occupational Science, 18(4), 292-305.
Helmer, Janet; Senior, Kate; Davison, Belinda & Vodic, Andrew (2015). Improving sexual health for young people: Making sexuality education a priority. Sex Education, 15(2), 158-171.
Horne, Felicity (2011). Conquering aids through narrative: Longlife positive HIV stories. English Studies in Africa, 54(2), 71-87.
Huber, Machteld; Knottnerus, André; Green, Law; Horst, Henriëtte van der; Jadad, Alejandro R.; Kromhout, Daan & Smid, Henk (2011). How should we define health? BMJ, 343(7817), 235-237, http://www.bmj.com/bmj/section-pdf/187291?path=/bmj/343/7817/Analysis.full.pdf [Accessed: December 5, 2017].
Kincheloe, Joe L. (2001). Describing the bricolage: Conceptualizing a new rigor in qualitative research. Qualitative Inquiry, 7(6), 679-692.
Lee, Juliet P.; Kirkpatrick, Sean; Rojas-Cheatham, Ann; Sin, Talaya; Moore, Roland S.; Tan, Sotheavy & Ercia, Angelo (2016). Improving the health of Cambodian Americans: Grassroots approaches and root causes. Progress in Community Health Partnerships: Research, Education, and Action, 10(1), 113-121.
Lincoln, Yvonna S. & Guba, Egon (2013). The constructivist credo. Walnut Creek, CA: Left Coast Press.
Linell, Per (2009). Rethinking language, mind, and world dialogically. Charlotte, NC: Information Age Publishing.
Ludlow, Bryn A. (2014). Witnessing: Creating visual research memos about patient experiences of body mapping in a dialysis unit. American Journal of Kidney Diseases, 64(5), A13-A14.
MacGregor, Hayley (2009). Mapping the body: Tracing the personal and the political dimensions of HIV/AIDS in Khayelitsha, South Africa. Anthropology & Medicine, 16(1), 85-95.
MacGregor, Hayley & Mills, Elizabeth (2011). Framing rights and responsibilities: Accounts of women with a history of AIDS activism. BMC International Health and Human Rights, 11(3), S7, https://doi.org/10.1186/1472-698X-11-S3-S7 [Accessed: August 27, 2016].
Maina, Geoffrey; Sutankayo, Lynn; Chorney, Raymond & Caine, Vera (2014). Living with and teaching about HIV: Engaging nursing students through body mapping. Nurse Education Today, 34(4), 643-647.
Mitchell, Lisa M. (2006). Body and illness: Considering Visayan Filipino children's perspectives within local and global relationships of inequality. Medical Anthropology, 25(4), 331-373.
Murasaki, Aryel K. & Galheigo, Sandra M. (2016). Juventude, homossexualidade e diversidade: Um estudo sobre o processo de sair do armário usando mapas corporais. Cadernos de Terapia Ocupacional da UFSCar, 24(1), 53-68, https://doi.org/10.4322/0104-4931.ctoAO0648 [Accessed: November 27, 2017].
Napier, A. David; Ancarno, Clyde; Butler, Beverley; Calabrese, Joseph; Chater, Angel; Chatterjee, Helen; Guesnet, François; Horne, Robert; Jacyna, Stephen; Jadhav, Sushrut; Macdonald, Alison; Neuendorf, Ulrike; Parkhurst, Aaron; Reynolds, Rodney; Scambler, Graham; Shamdasani, Sonu; Smith, Sonia Z.; Stougaard-Nielsen, Jakob; Thomson, Linda; Tyler, Nick; Volkmann, Anna-Maria; Walker, Trinley; Watson, Jessica; Williams, Amanda C. de C.; Willott, Chris; Wilson, James & Woolf, Katherine (2014). Culture and health. The Lancet, 384(9954), 1607-1639, https://doi.org/10.1016/S0140-6736(14)61603-2 [Accessed: September 22, 2016].
Nöstlinger, Christiana; Loos, Jasna & Verhoest, Xavier (2015). Coping with HIV in a culture of silence: Results of a body-mapping workshop. AIDS Research and Human Retroviruses, 31(1), 47-48.
Núñez-Pacheco, Clausia & Loke, Lian (2016). Felt-sensing archetypes: Analysing patterns of accessing tacit meaning in design. In Callum Parker, Haifeng Shen, Eunice Sari (Eds.), Proceedings of the 28th Australian Conference on Computer-Human Interaction (pp.462-471). New York: ACM.
Oliveira, Elsa; Meyers, Susan V. & Vearey, Jo (Eds.) (2016). Queer crossings: A participatory arts-based project, https://issuu.com/move.methods.visual.explore/docs/queer_crossings_publication_v.2_-_f [Accessed: August 27, 2016].
Orchard, Treena (2017). Remembering the body. Ethical issues in body mapping research. Cham: Springer.
Orchard, Treena; Smith, Tricia; Michelow, Warren; Salters, Kate & Hogg, Bob (2014). Imagining adherence: Body mapping research with HIV-positive men and women in Canada. AIDS Research and Human Retroviruses, 30(4), 337-338.
Parker, Patricia; Holland, Dorothy; Dennison, Jean; Smith, Sarah H. & Jackson, Melvin (2017). Decolonizing the academy: Lessons from the graduate certificate in participatory research at the University of North Carolina at Chapel Hill. Qualitative Inquiry, Online first.
Pithouse-Morgan, Kathleen; Naicker, Inbanathan; Chikoko, Vitallis; Pillay, Daisy; Morojele, Pholoho & Hlao, Teboho (2014). Entering an ambiguous space: Evoking polyvocality in educational research through collective poetic inquiry. Perspectives in Education, 32(4), 149-170.
Quijano, Angela & Vieira, Adriane (2016). A experiência da dor lombar como condição crônica em mulheres trabalhadoras da cooperativa do assentamento rural "Filhos de Sepé". In António Pedro-Costa, Catarina Brandão, Jaime Ribeiro, Francislê Neri de Souza & Dayse Neri de Souza (Eds.), Atas 5º Congresso Ibero-Americano em Investigação Qualitativa CIAIQ2016, 2(0) (pp.1286-1291), http://proceedings.ciaiq.org/index.php/ciaiq2016/article/view/885 [Accessed: August 16, 2016].
Ramsuran, Anitha & Lurwengu, Fikile (2008). Relations of power in different spaces: An exploration of the schooling experiences of children in an HIV/AIDS context. Journal of Psychology in Africa, 18(3), 393-399.
Rose, Gillian (2006). Visual methodologies: An introduction to interpreting visual materials (2nd ed.). London: Sage.
Ross-Quiroga, G. Violeta (2013). Yo, tú, nosotras: Huellas de la violencia y el sida en la corporeidad e identidad de las mujeres viviendo con VIH, las trabajadoras sexuales y las mujeres trans de tres ciudades de Bolivia, http://onusidalac.org/1/images/2013/04-abril/138328495-Estudio-Violencia-en-Tres-Poblaciones-de-Mujeres-en-Bolivia.pdf [Accessed: August 28, 2016].
Santos, Boaventura de Sousa (2004). The world social forum: Toward a counter-hegemonic globalisation (Part I). World Social Forum: Challenging Empires, 233-245, http://www.boaventuradesousasantos.pt/media/wsf_JaiSenPart1.pdf [Accessed: November 27, 2017].
Santos, Boaventura de Sousa (2007a). From an epistemology of blindness to an epistemology of seeing. In Boaventura de Sousa Santos (Ed.), Cognitive justice in a global world: Prudent knowledges for a decent life (pp.407-438). Lanham: Lexington Books.
Santos, Boaventura de Sousa (2007b). A Discourse on the sciences. In Boaventura de Sousa Santos (Ed.), Cognitive justice in a global world: Prudent knowledges for a decent life (pp.13-45). Lanham: Lexington Books.
Santos, Boaventura de Sousa (2015). Epistemologies of the South: justice against epistemicide (pp.152-153). London: Routledge.
Santos, Boaventura de Sousa; Araújo, Sara & Baumgarten, Maíra (2016). As epistemologias do sul num mundo fora do mapa. Sociologias, 18(43), 14-23, https://doi.org/10.1590/15174522-018004301 [Accessed: November 27, 2017].
Senior, Kate; Helmer, Janet; Chenhall, Richard & Burbank, Victoria (2014). "Young clean and safe?" Young people's perceptions of risk from sexually transmitted infections in regional, rural and remote Australia. Culture, Health & Sexuality, 16(4), 453-466.
Shumka, Leah & Benoit, Cecilia (2007). Social suffering and gaps in alternative health care for vulnerable women workers. In Jennie Jacobs Kronenfeld (Ed.), Inequalities and disparities in health care and health: Concerns of patients, providers and insurers (pp.253-275). Oxford: Elsevier.
Silva, Jimena (2013). Con-textos y cuerpos situados. In Jimena Silva & Leyla Méndez (Eds.), Cuerpos y metáforas. Estudio de los significados culturales del cuerpo y las sexualidades juveniles (pp.40-79). Antofagasta: Universidad Católica del Norte.
Silva, Jimena & Méndez, Leyla (Eds.) (2013). Cuerpos y metáforas. Estudio de los significados culturales del cuerpo y las sexualidades juveniles. Antofagasta: Universidad Católica del Norte.
Smit, Warren; de Lannoy, Ariane; Dover, Robert V.H.; Lambert, Estelle V.; Levitt, Naomi & Watson, Vanessa (2016). Making unhealthy places: The built environment and non-communicable diseases in Khayelitsha, Cape Town. Health & Place, 39, 196-203, https://doi.org/10.1016/j.healthplace.2016.04.006 [Accessed: November 27, 2017].
Smith, Linda Tuhiwai (2012). Decolonizing methodologies: Research and indigenous peoples (2nd ed.). London: Zed Books.
Solomon, Jane (2007). "Living with X": A body mapping journey in time of HIV and AIDS. Facilitator's guide. Johannesburg: REPSSI.
Stevens, Marion & Le Roux, Nicole (2011). A human rights violation: The forced sterilization of HIV positive women. Nursing Update, 35(3), 32-35.
Suri, Harsh (2011). Purposeful sampling in qualitative research synthesis. Qualitative Research Journal, 11(2), 63-75.
Sweet, Elizabeth L. & Escalante, Sara O. (2015). Bringing bodies into planning: Visceral methods, fear and gender violence. Urban Studies, 52(10), 1826-1845.
Trust for Indigenous Culture and Health (2015). Our positive bodies. Mapping our treatment, sharing our choices, http://ticahealth.org/?p=1 [Accessed: September 19, 2016].
Van de Riet, Mary; Hough, Angela & Bev, Killian (2005). Mapping HIV/AIDS as a barrier to education: A reflection on the methodological and ethical challenges to child participation. Journal of Education, 35(1), 75-98.
Ward, Nicola; Nabwire, Jacqueline; Magero, Jacinta & Biryeteg, Annet (2006). Memory work: Learning from the Ugandan experience, http://www.bibalex.org/Search4Dev/files/292432/122956.pdf [Accessed: August 15, 2016]
Wienand, Annabelle (2006). An evaluation of body mapping as a potential HIV/AIDS educational tool. CSSR Working Paper, 169, https://open.uct.ac.za/handle/11427/19328 [Accessed: November 27, 2017].
World Health Organization (2017). WHO | Health Research Systems Analysis (HRSA) concepts and indicators, http://www.who.int/rpc/health_research/concepts/en/ [Accessed: April 4, 2017].
Denise GASTALDO is an associate professor, Faculty of Nursing and School of Public Health, University of Toronto, Canada, and director of the Centre for Critical Qualitative Health Research at the same institution. Her scholarship focuses on health equity, in particular she studies migration and gender as social determinants of health in Canada and Ibero-America.
Contact:
Dr. Denise Gastaldo
University of Toronto
155 College Street, suite 130, Toronto, M5T 1P8
Canada
E-mail: denise.gastaldo@utoronto.ca
http://www.ccqhr.utoronto.ca/graduate-education/instructors-and-bios/denise-gastaldo
Natalia RIVAS-QUARNETI is an occupational therapy assistant professor, University of A Coruna, Faculty of Health Sciences, Spain, and honorary lecturer at Brunel University London, United Kingdom. Her work focuses on critical approaches to occupation, health, and well-being, with special attention to people and communities living vulnerable situations and participatory methodologies.
Contact:
Dr. Natalia Rivas-Quarneti
University of A Coruna, Faculty of Health Sciences
Campus de Oza s/n C.P. 15006 A Coruña
Spain
E-mail: natalia.rivas.quarneti@udc.es
ORCID iD: http://orcid.org/0000-0001-9444-4347
Lilian MAGALHÃES is an adjunct professor, Occupational Therapy Department, Federal at University of Sao Carlos, Brazil and professor emerita, Western University of Ontario, Canada. Her work is geared toward the development of anti-racist and emancipatory research approaches, especially art-based methodologies.
Contact:
Dr. Lilian Magalhães
Federal at University of Sao Carlos, Occupational Therapy Department
Rod. Washington Luis, km 235, São Carlos
Brazil
E-mail: lmagalhaes@ufscar.br
ORCID iD: http://orcid.org/0000-0003-3666-3685
Gastaldo, Denise; Rivas-Quarneti, Natalia & Magalhães, Lilian (2018). Body-Map Storytelling as a Health Research Methodology: Blurred Lines Creating Clear Pictures [60 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 19(2), Art. 3, http://dx.doi.org/10.17169/fqs-19.2.2858.

Creative Commons Attribution 4.0 International License