Volume 19, No. 1, Art. 6 – January 2018
The General Practice Health Waiting Area in Images: Threshold, Borderland, and Place of Transition in the Sense of Self
Gary Clapton
Abstract: The waiting rooms and areas of general practice (GP) health facilities are places that nearly all of us will find ourselves in but the waiting experience is under-explored. What happens to our sense of self when we move between the outside world where we are citizens and these spaces where we become patients-in-waiting? I begin with what has been written about waiting in general and in health waiting areas in particular. I then discuss a photo-documentation study of twenty-two GP waiting rooms in Edinburgh, Scotland and explore the questions that arise from the resultant images.
Examples are presented that illustrate the unique place of the waiting room in the patient journey between the outside world and the encounter with their doctor. Examples are given of both calm-inducing and unsettling elements. Potentially disempowering processes are identified occasioned by the waiting experience and the issue of the transition in sense of self is raised. I conclude by pointing to other waiting areas and places where such dynamics and processes might be more acute.
Key words: waiting; waiting experience; calming and unsettling; agency; docility; thresholds; from citizen to patient; supplicant status; photo-documentation
Table of Contents
1. Introduction
2. Waiting
3. Health Waiting Areas
4. The Study
4.1 Methodological frameworks
4.2 Data analysis
5. Waiting for the Doctor: The General Practice Health Waiting Area in the Frame
5.1 Waiting: Agitating, calming, worrying
5.2 Waiting: The encouragement of docility and the shift from citizenship
6. Discussion
In this article I report on and discuss research that photo-documented twenty-two health waiting areas, with specific attention to the nature of waiting in these places. Implications for content and design are offered and the nature of waiting for other public services is highlighted for attention. [1]
Waiting has been shortened, and continued effort is spent on seeking to abolish it altogether. We need no longer wait for a bus, sports results come in as they happen, most photographs don't have to be collected from the developers and there is no need for cheque clearance when money can be transferred between accounts in seconds. [2]
Not all forms of waiting have been done away with; a red traffic light means stop and wait, plumbers are still late, exam results are still awaited, Santa Claus will not arrive before 25th December, blood tests still take time. The need to exercise patience has been reduced, not a bad thing if this means less dread or anxiety. And there is pleasurable waiting that is nearer to anticipation (and cannot be hurried): waiting for the birth of a child, for example. Drawing on a study of general practice health waiting areas in Scotland that uses photo-documentation as a research method, in this article I offer thoughts on waiting in general, and focus specifically on the experience of waiting to see a doctor. [3]
If "waiting is a universal experience that everyone can describe in some personal way in relation to their own lives" (BOURNES & MITCHELL, 2002, p.58), it is surprising, as will be seen, that so little has been written about the experience. [4]
I will begin with a discussion of what has been written about waiting in general (Section 2). After that, I discuss what we know about waiting in health waiting areas (Section 3). This will be followed by an account of the methodology of the study (Section 4). Section 5 presents my findings and analysis, leading to a discussion and conclusion (Section 6). [5]
The philosopher TALLIS, while noting that there are countless forms of waiting, from the ecstatic to the unbearable, observes that "[w]aiting reflects our helplessness, our inability to control the pace as well as the course of events" (2013, p.48). Sociologist SCHWARTZ (1974) points to the degradational aspects of being kept idle that are intrinsic to waiting. Psychologist LEVINE (1987) configures waiting as the experience of loss (of control). Noting that waiting is under-theorised and under-researched, and that few like to wait, BISHOP, writing from the standpoint of an architect, quotes MULCAHY, PARRY and GLOVER who consider that waiting puts "people at the mercy of another's schedule" (2010, p.1063). His description of waiting is damning:
"... much waiting is still pervaded by a sense of the prosaic or banal, whether or not this banality is inculcated through 'entertainment' or opportunities for consumption, by programmed 'hospitality' and through other distractions, by deliberate architectural design, or just by a general sense of tedium" (BISHOP, 2013, p.141). [6]
BISHOP uses the word "sump" to describe waiting zones, and includes camps for refugees and asylum seekers as well as "more prosaic micro-waiting sites associated with social services, public medical facilities, or the social justice system" (ibid.). SCHWEIZER, is brief: "Waiting has neither form, nor goodness, nor beauty" (2005, p.789). Even MILTON the poet suggests that waiting is rarely actively chosen: "They also serve who only stand and wait” (1991 [1673], p.81). [7]
BISSELL (2007) is one of the few writers with an alternative, more optimistic, approach to waiting. He argues that waiting can be a creative process if seen not as "the immobile being-in-the-world that it first appeared" (p.295), but rather "thought of as a period of incipient rich duration" (ibid.). BISSELL argues that "the dominant mode of being in the world may not necessarily be one of sustained engaged activity" (p.281), and instead finds potential richness in waiting transformed as a type of positive patience in which the person who waits retains and exercises agency recalibrating the experience from one of potential squandered time to that of a period of nourishing calm. [8]
In between the two poles of waiting as time to be endured or enjoyed, there are a variety of experiences that are time and place-dependent, and unforeseen, e.g., sudden delays in travel arrangements. Any given experience of waiting might be both endured and enjoyed. Increasingly such experiences are used as opportunities for professional and personal social media activity, including attending to e-mails or reading reports (BERRY & HAMILTON, 2010) as well as checking Facebook, gaming, and catching up on the news. In relation to the latter, DIMMICK, FEASTER and HOPLAMAZIAN (2010) suggest that some waiting periods, especially the unanticipated, can be considered as "interstices" in people's daily schedules that may be put to good use by smartphones. However the consensus in the sparse literature that exists on the act of waiting is that time spent waiting is wasted time. It is an experience that is not actively sought out, and one that has the capacity to disempower. How much of this is applicable to the specific event of health care waiting? RITTENMEYER, HUFFMAN and GODFREY's systematic review is scathing about the waiting experience
"... waiting is a fearful, turbulent experience and one in which the healthcare system affords patients, families and/or significant others little opportunity to have the power to influence time and outcomes… A disconnect exists between healthcare system providers and patients, families and/or significant others regarding the meaning of waiting. For those who work in healthcare waiting is part of the culture, and is considered routine and normalized. For those who must wait the waiting is personal, fearful, and sometimes tortuous" (2014, p.218). [9]
How does the effect of the surroundings in which this waiting occurs either exacerbate or ameliorate the experience of those who must wait? [10]
"The medical waiting room is marked by literal and symbolic assaults on autonomy" (TANNER, 2002, p.117).
The health waiting area literature has generally concentrated on the "cosmetics" of place to make the wait more comfortable, including colour schemes, access to light, and views of nature (see ANDRADE & DEVLIN, 2015 for a review of the literature). A few writers have delved into the dynamics produced when space, place, and waiting meet.1) [11]
EVANS and McCOY offer a comprehensive discussion of the interior design of health facilities from an architectural perspective. Especially interesting is their notion of "misaffordances" (1998, p.88) in places, i.e., when design can create ambiguity or confusion of function or purpose resulting in disorientation. The consequence is that, "human reactions are likely to encompass frustration, annoyance, and, on occasion, even hostility or helplessness" (ibid.). This last echoes TALLIS (2013) on helplessness. BECKER and DOUGLASS point to the emotions that can be engendered during waiting, and point to the most common methods of ameliorating these:
"Depending on the nature, and circumstances of the wait, the 3 phases of waiting (preprocess, inprocess, and postprocess) can result in 2 basic psychological and physiological responses: uncertainty, including annoyance, irritability, and stress; and anger. To reduce these responses, health facilities typically provide some form of distraction, most often magazines, occasionally television, in the waiting space" (2008, p.130). [12]
Writing about stress reduction in hospital rooms, ANDRADE and DEVLIN (2015) note that "... a sense of control is related to opportunities to modify or alter aspects of the environment" (p.126). This might include, for instance, the ability to turn up the heating or open a window. However, distractions, colour schemes, and seating plans can only go so far. SIME reminds us that the manipulation of environment has a limit, and that human agency is a defining element in how spaces are used: "An individual, in creating a place, is involved by definition in the appropriation and personalization of a physical space through thought and action" (1986, p.60). [13]
The loss of control may be occasioned by the visit itself as the citizen is transformed into a patient who passively waits (and endures?—the root of "patient" is the Latin for suffering). LEATHER, BEALE, SANTOS, WATTS and LEE note that the stress associated with attending for medical treatment can also be accompanied by feelings of loss of the control that ordinarily is exerted over many aspects of daily life, including control over the physical environment, but is to a certain degree relinquished by the visit (2003, p.845). FOGARTY and CRONIN talk of feelings of uncertainty and powerlessness bound up with the "anticipation of a response to the healthcare need" (2008, p.463), and in their study, BOURNES and MITCHELL describe waiting as "a gruelling experience of unsure stillness" (2002, p.62). Quite apart from the continuing debates over the power imbalance between GP and patient (GREENHALGH, SNOW, RYAN, REES & SALISBURY, 2015), it seems that there is something in this kind of waiting itself, before any meeting, that can result in uncertainty, feelings of disempowerment, and loss of agency. However, such relinquishment of individual power occasioned in the waiting period is only implicit in the many discussions of the need for distractions, less illness-focused environments, and general efforts to make the waiting time calmer. [14]
Also absent from the literature on health waiting areas is consideration of how these may be differently experienced depending upon the reason for being there. Most of the literature relates to those who are unwell, whereas the happily expectant mother might be content to wait, somewhat oblivious of her surroundings, for pleasurable knowledge of her child (although there are limits to everyone's patience). More nuanced studies are also needed on the difference in experiences of waiting between those who are frequent and first-time visitors. There is also a dearth of literature on culturally conditioned attitudes and behaviours in health waiting areas (NOESJIRWAN, 1977). ARNEILL and DEVLIN's (2002) study appears to be the only one that uses photographs of waiting rooms to elicit patient views and assessments relating to whether the image viewed depicted (and predicted) quality of care, i.e., images that invoked a dull and unwelcoming impression equated with speculation that the care to come would be similarly unsatisfactory (see below). Thus, although some attention has been given to "the importance of 'place' in the organization of health care" (STREET & COLEMAN, 2012, p.10), there seems to be a dearth of writing on the socio-spatial environment of health waiting areas, their "atmospherics" (TSAI et al., 2007, p.1), and what NEUWELT, KEARNS and BROWNE term "the complex but under-recognised internal geographies" (2015, p.288) of these spaces and places. [15]
In the summer of 2015 I was part of a collaboration between the University of Edinburgh, the National Health Service, and a photographer. My work on the way that fathers were depicted in publicity for children and family services (CLAPTON, 2013), attracted the attention of a health promotion expert who was interested in improving the way that health promotion materials in general practice surgery waiting areas could better reflect gender balance. After discussion, the result was a plan to create a series of photographs of general practice health centre waiting areas and rooms. Quantity was a priority in order to generate as full an impression as possible. We thus adopted a convenience sampling approach that entailed contacting all listed health centres in the city, with a view to researching their health publicity materials (SAUMURE & GIVEN, 2008). Permission to photograph was given in the case of twenty two health centres when the waiting areas were empty. This number is over a quarter of all general practice health centres in a large city and as such provides a representative sample of what might be expected in the others. During and after a pilot shoot, it became clear that there was much more of interest than just health promotion posters and leaflets. More specifically, the question "What were these areas like to wait in?" emerged. PETERSEN and ØSTERGAARD argue that:
"In the knowledge society we primarily focus on turning the unknown into something known with the purpose of becoming more knowledgeable and improve our qualifications. When using the photos the idea is reverse: to show known surroundings and ways of acting in a different context and thereby spur new ways of looking upon things we otherwise do without paying particular attention" (2003, p.5). [16]
So in this spirit of a new way of looking, all twenty-two waiting areas were systematically photographed. The outsides and entrances, walls, floors, table tops, reception counters and desks were photographed by a qualified photographer using a single camera and accompanied by myself. Obscure nooks and crannies were not photographed, nor were photographs taken from the perspective of the receptionists or other staff, e.g., those behind a desk. Rather we photographed what the eye of someone waiting to use the service would see, whether they were standing or seated. Notices, leaflets, instructions and other reading materials were photographed in close-up so as to be legible for the research in the same way that they might be read by those who were waiting. [17]
In all, 800 images were produced, and what follows is a combination of thoughts provoked by both the experience of undertaking the work and the images themselves, with commentary on selected images. [18]
As noted above the scope of the research widened to become a more open-ended inquiry into the waiting room as a place which influences people's experiences of visiting their doctor. The working research question became: "What factors within and around the health service waiting room might determine or influence the patients' waiting experience?" [19]
To my knowledge there has only been one other work that has used photographic means to "get at" what it might feel like to wait in a health facility waiting area. This was undertaken in the USA, and the images were subsequently used to stimulate conversations with those who use the facilities (ARNEILL & DEVLIN, 2002). As noted above, the research was image-based only, generated when the waiting rooms were empty of patients. [20]
The physical nature of our process of data collection meant that sounds (TV, radio), lighting (natural and artificial) and impressions (overall welcoming "feel" or otherwise) were part of, and influenced, the process of the research. Sensory information such as sound and lighting has been omitted, but some bias may be present about whether a given place felt welcoming and comfortable. [21]
It is acknowledged that in the words of BUCHANAN, "the resultant images may reveal more about the photographer than the photographed" (2001, p.162), and as such the decisions as to where to point the camera could not be objective (HARPER remarks that "all images are socially and technically constructed", [1994, p.406]). Thus the research process, as for much social science research, though reflexive, cannot claim to be objective. Importantly, PINK observes that
"... images have no fixed or single meanings and are not capable of capturing an objective reality. The most one can expect is that observation and images will allow one only to interpret that which is visible and the other elements of experience that are evoked through this" (2007, p.32). [22]
PAUWELS echoes this view of visual representations having no fixed meaning and argues that the value of images lies in their combination with a given purpose and research question, and "a sound process of going from visual facts or indications to a reasoned and substantiated set of inferences" (2011, p.9). [23]
PAUWELS' idea of photographs as "windows" to the depicted world (p.5) provided the basis for an exploratory search for patterns: "Pattern recognition begins with the anthropologist's inspecting a series of things, field notes, or other fieldwork documents, including photographs and audiotapes, and abstracting from them one or more general features recognized in the event" (HONIGMAN, 1976, p.248). In this respect searching for patterns in the images echoes the classic thematic analytical approach of seeking to identify repetitive features or themes so as to discern patterns (BOYATZIS, 1998). BRAUN and CLARKE's discussion on the uses of thematic analysis is useful to note here. They counsel caution on the blanket use of the approach, noting, for instance that patterns do not necessarily emerge on the basis of, for example, frequency, and suggest that "the 'keyness' of a theme is not necessarily dependent on quantifiable measures—but in terms of whether it captures something important in relation to the overall research question" (2006, p.82). They also go on to argue that themes do not emerge independently but instead develop as a result of the active role of the researchers who bring their own values and interests to the table. That is, in the words of KNOBLAUCH, BAER, LAURIER, PETSCHKE and SCHNETTLER, "looking at" means "being framed by" (2008, §9). This is especially pertinent when, as in this study, there are no other perspectives included (e.g., those of the waiting members of the public, whose experience of the waiting areas might change according to their mood on the day, or those of the staff whose experiences will be different from the public because of role and the influence of organizational issues such as time-management). So, to make the research aim more explicit, the implicit assumption in exploring the factors within and around the health service waiting room that determine or influence the patients' waiting experience was derived from a developing understanding that the waiting experience in health service areas had not only been under-researched but was a potentially fraught one that could be made better. [24]
We therefore acknowledge that the general features of the waiting areas identified by the research team are open to multiple readings by others. However, we believe that the clear research question, the rigour in data (images) collection, the transparency of purpose and the resonance that can be found between observations about the images and the existing literature on waiting and waiting in health areas offer a sufficient degree of legitimacy to the following observations about the waiting experience in health waiting areas. [25]
5. Waiting for the Doctor: The General Practice Health Waiting Area in the Frame
Other researchers have previously generated suggestions about improving the waiting experience (CLAPTON & REID, 2017). In this article, I turn to the data to make broader theoretical observations about health waiting areas and citizenship. As such, BISSELL's admonition to think twice before seeking to "fix" things about the waiting experience is worth bearing in mind, for example by trying to make time spent waiting more productive (2007, p.294). Figure 1 is an image that illustrates the type of waiting rooms that were photographed.

Figure 1: Door to general practice waiting room [26]
So here, in keeping with HONIGMAN's notion of "pattern recognition" (1976, p.245), two elements generated from study of the images collected are identified, that when taken together, allow a more theoretical interrogation of the processes and dynamics that might be in operation when we visit the doctor. [27]
The first of the elements consists of a collection of features that, we suggest, can either reduce anxiety or unsettle the person that waits. [28]
5.1 Waiting: Agitating, calming, worrying
"Agitated" and "calming" can be subjective descriptions and this emergent category of the data can be considered as having "latent content" (ROBSON, 2016, p.354), that is, content that is not manifest but implicit and is the result of interpretation by the research team, with the provisos about researcher bias already discussed. [29]
A minority of the images emanated calmness in showing windows to gardens or greenery, lightness, and airiness. Images of waiting areas in this category also included plants, fish tanks, individual touches such as book lending libraries, local art, and other connections with the surrounding community such as cooking recipe books for sale.

Figure 2: Light and airy

Figure 3: Fish tanks [30]
Images that tended to agitate the sight were of waiting rooms that were overstocked or cluttered with leaflets and posters, had high televisions that were either switched off, unplugged, featured sound-off "rolling news", or were switched to static, radios playing "muzak" (e.g., "drive-time" radio or tinny pop), and other features such as "Speak Here" grilles to communicate with the receptionist.

Figure 4: High-up and switched to static [31]
On studying the images, what was striking, for want of a better phrase, was a "white noise" for the eyes—a large number of leaflets and posters, in some cases covering most available walls.

Figure 5: "White noise" for the eyes [32]
On careful study of the images, the many times that posters and leaflets in the waiting rooms featured the words "worry", "anxious", "concern" or "problem" was also noticeable. This echoes a concern expressed by GIGNON, IDRIS, MANAOUIL and GANRY (2012) as to the possibility that some display materials could provoke anxiety. The amount of information was staggering with its mix of "five-a-day" tips, rape crisis information, asthma helplines, neighbourhood watch warnings, local tea dance news, Ebola virus updates, and so on. But the more obvious potential provokers of discomfort were lurid posters of the shock-content type that depicted the threats or ravages of disease.
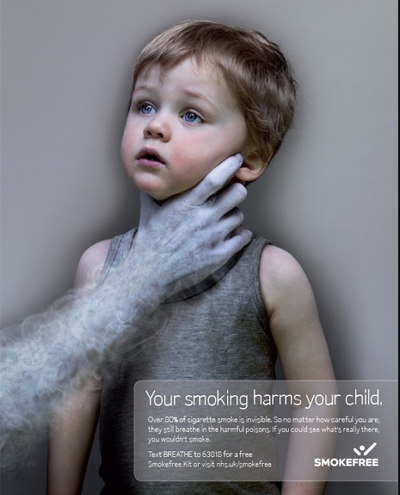
Figure 6: Example of shock content [33]
Based on the images, we conclude that, while there were calm-inducing elements in nearly all the waiting rooms, there was no one waiting room that could be confidently assessed as a place that was agitation-free, where time might be passed relatively untroubled. We speculate that while waiting in such surroundings, the temptation to “switch off”, and to “switch on” or self-immerse in social media, must be a powerful one. [34]
5.2 Waiting: The encouragement of docility and the shift from citizenship
TANNER describes the medical waiting room as a "liminal space" and that "time spent in a waiting room represents time wasted" (2002, p.116). For her, the waiting room (temporarily) limits the ability to exercise the range of actions that would be expected on the "outside" (even the use of social media may be discouraged or disallowed): "the waiting room symbolically impairs even its healthy occupants" (p.122). She finds negative signals in the magazines of the waiting room:
"Although these magazines promise a bridge to the narrative world outside the waiting room, they ultimately emphasize the reader's exclusion from that world; as time in the waiting room is emptied of its 'news' function, 'reading for the plot' loses much of its pleasure. Someone waiting may feign interest in old stories, but thumbing through 'tattered and worn' magazines marks exclusion from a world in which new narratives are constructed, and consumed" (p.123). [35]
In the present study, images of sight lines that included banks of case files and obscured reception staff, i.e., behind computer screens, lent an impersonal quality to the visual environment. The unattractiveness of the sight of files has appeared in the literature (LEATHER et al., 2003), however there may be more at work here than aesthetics.
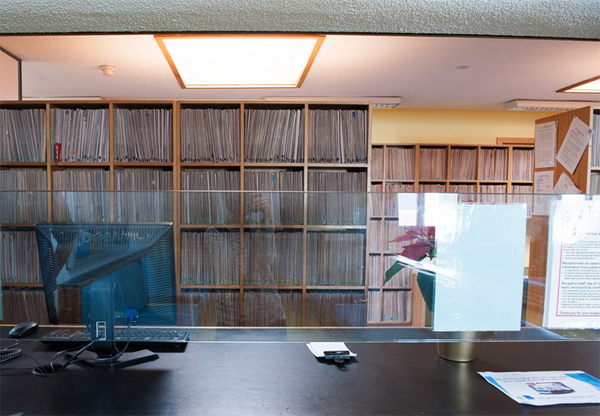
Figure 7: Banks of files [36]
The sight of banks of case files can engender an oppressive atmosphere, one aspect described by GOODSELL, writing about public service waiting areas as "Kafkaesque" (1984, p.471). [37]
The notices that were depicted were often instructional in tone, talking at the reader with a list of dos and don'ts ("Could all patients please refrain from ..."). Other notices reminded the reader that "CCTV surveillance was in operation"2). In one location, information about the "dos" and "don'ts" type was placed high up on the walls and was in small print. Whether "No Smoking" signs were still called for was also a question. The number of "shouty" admonishing instructions, sometimes written in red and bolded, far out-weighed the more soothing or facilitative type that carried information about breast-feeding or baby-changing on the premises.
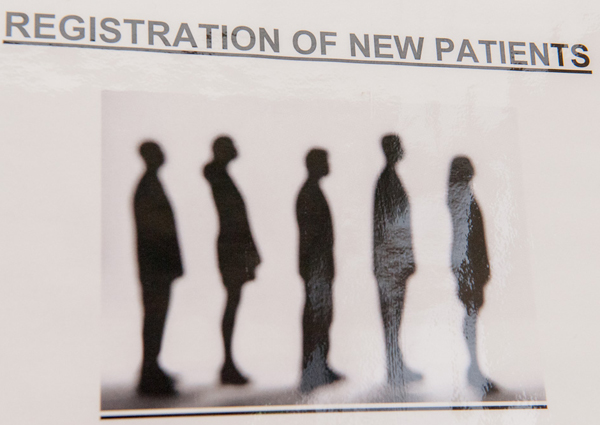
Figure 8: Registration of new patients [38]
Health waiting areas that contain little trace of the world outside their doors are both borderlands that face inwards to "patienthood" and outwards to citizen status. They are "liminal, in-between, and initiatory places" (BISHOP, 2013, p.140). Crossing the thresholds of the health waiting areas from the street can inculcate a feeling of entering a place for recipients of treatment and a helplessness-inducing experience. Before the advent of a national health service in the UK, doctors' services had to be purchased, debts could be incurred, and there was no sense of a broad entitlement to help with illness. The result was that the transaction between doctor and patient was one characterised by a dynamic of supplicant (patient) and provider (doctor). This relationship is graphically depicted in LOWRY's painting of a doctor's surgery waiting room in the 1930s. The figure on the left stares out at us, cap-in-hand, the perfect image of the supplicant or beggar.
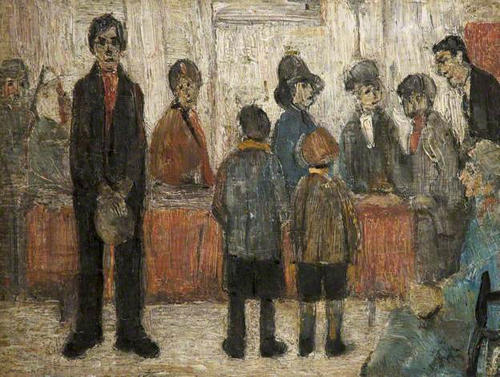
Figure 9: "A Doctor's Waiting Room" (The L.S. Lowry Collection) [39]
The process of entering a general practice health service waiting room is that of entering a world apart from ordinary lives. Some of the literature indicates this, and in some settings, considerable effort is made to reduce the feelings of disempowerment and discomfort that attend this process. My findings suggest that it remains the case that the health waiting room environment has the potential to encourage passivity and increase anxiety and produce a retreat into, in both senses of the phrase, a patient silence. The transition from citizen to patient contains disempowering potential. It is an identity shift akin to what GOTTDIENER (2001) talks of, in the context of using airports, as experiencing a transition from passenger to consumer (although in his particular example, agency and citizenship are retained, rather than diminished). [40]
It is not only health service waiting areas that have been neglected as a topic of inquiry; public service waiting areas as a whole have received little attention. The waiting experiences in areas as diverse as unemployment offices, asylum application centres, criminal court waiting rooms, social work reception areas and sexual health clinics have been under-researched. Arguably the shift in identity towards that of a supplicant is much greater in areas where we wait to find employment or proceed through the asylum-claim system. In these places, and the others referred to above, the very reason for being there can provoke feelings of anxiety. However, this research suggests that the atmosphere of place, the out-of-date leaflets, the shouting nature of instructional posters, and other visual markers identified here, can combine to intensify the unbearable nature of the waiting experience in these places. [41]
In conclusion, I have argued that the surroundings in which we wait for a health service can ready us for a two-way conversation with a clinician, or render us passive. I also suggest that the surroundings in which we wait for public services are often considered as proxies for the quality of service that will be received. Poorly ordered surroundings might betoken a poor service, while care taken with design, content and general atmosphere may reassure the person who waits that they will be cared for. [42]
Further studies could explore with GPs and their staff how these places are constructed and experienced by them, thus boosting knowledge of the internal geographies of health waiting areas and awareness about their potential impact on feelings, sensibilities, and moods. In addition to those limitations already noted (such as the subjective nature of aspects of the study methodology), I have not specifically discussed waiting areas in relation to the differing experiences and needs of particular demographic groups. Neither is the sample large enough to make generalisations. Rather it is hoped that this article will provide food for thought, stimulate discussion, and lead the way to further research. [43]
This study was made possible with the co-operation of NHS Lothian and the managers of twenty-two General Practice Health waiting rooms. The initial idea was that of Lesley REID, of NHS Lothian. The photography was undertaken by Kinga KOCIMSKA in the case of images 1-5, and 7-8. Image 6 is from a photograph by myself. Image 9 is reproduced by permission of by ArtUK.
1) Debates about the differences, overlaps and similarities between the concepts of space and place are many (LOW, 2016). The working definitions I used in this article are that of AGNEW on place as a setting "where everyday life activities take place" (2009, p.36) and LEFEBVRE's notion of space: "space is never empty: it always embodies a meaning" (1991, p.154). That is to say, "place" here is used as a locality, an address, and space used as a place where things happen, where the contents, design etc. of place and people interact with each other. <back>
2) CCTV: Closed Circuit Television <back>
Agnew, John (2009). Globalization and sovereignty. Lanham, MD: Rowman and Littlefield.
Andrade, Claudia C. & Devlin, Ann S. (2015). Stress reduction in the hospital room: Applying Ulrich's theory of supportive design. Journal of Environmental Psychology, 41, 125-134.
Arneill, Allison B. & Devlin, Ann S. (2002). Perceived quality of care: The influence of the waiting room environment. Journal of Environmental Psychology, 22, 345-360.
Becker, Franklin & Douglass, Stephanie (2008). The ecology of the patient visit: Physical attractiveness, waiting times, and perceived quality of care. Journal of Ambulatory Care Management, 31(2), 128-141.
Berry, Marsha & Hamilton, Margaret (2010). Changing urban spaces: Mobile phones on trains. Mobilities, 5(1), 111-129.
Bishop, Peter (2013). Surveying "the waiting room". Architectural Theory Review, 18(2), 135-149.
Bissell, David (2007). Animating suspension: Waiting for mobilities. Mobilities, 2(2), 277-298.
Bournes, Debra A. & Mitchell, Gail J. (2002). Waiting: The experience of persons in a critical care waiting room. Research in Nursing & Health, 25(1), 58-67.
Boyatzis, Richard (1998). Transforming qualitative information: Thematic analysis and code development. Thousand Oaks, CA: Sage.
Braun, Virginia & Clarke, Victoria (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
Buchanan, David A. (2001). The role of photography in organization research. A re-engineering case illustration. Journal of Management Inquiry, 10(2), 151-164.
Clapton, Gary (2013). Social work with fathers. Edinburgh: Dunedin Press.
Clapton, Gary & Reid, Lesley (2017). Neglected spaces: UK general practice surgery waiting rooms. British Journal of General Practice Open, 1-11, http://bjgpopen.org/content/bjgpoa/1/1/BJGP-2017-0641.full.pdf [Accessed: October 1, 2017].
Dimmick, John; Feaster, John & Hoplamazian, Gregory (2010). The niches of interpersonal media: Relationships in time and space. New Media & Society, 13(8), 1265-1282.
Evans, Gary W. & McCoy, Janetta M. (1998). When buildings don't work: The role of architecture in human health. Journal of Environmental Psychology, 18(1), 85-94.
Fogarty, Caroline & Cronin, Patricia (2008). Waiting for healthcare: A concept analysis. Journal of Advanced Nursing, 61(4), 463-471.
Gignon, Maxime; Idris, Hadjila; Manaouil, Cecile & Ganry, Oliver (2012). The waiting room: Vector for health education? The general practitioner's point of view. BMC Research Notes, 5:511, 1-6, https://bmcresnotes.biomedcentral.com/articles/10.1186/1756-0500-5-511 [Accessed: October 1, 2017].
Goodsell, Charles (1984). Welfare waiting rooms. Journal of Contemporary Ethnography, 12(4), 467-477.
Gottdiener, Mark (2001). Life in the air: Surviving the new culture of air travel. Oxford: Rowman & Littlefield Inc.
Greenhalgh, Trisha; Snow, Rosamund; Ryan, Sara; Rees, Sian & Salisbury, Helen (2015). Six "biases" against patients and carers in evidence-based medicine. BMC Medicine, 13:200, https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-015-0437-x [Accessed: October 1, 2017].
Harper, Douglas (1994). On the authority of the image. In Norman K. Denzin & Yvonna S. Lincoln (Eds.), Handbook of qualitative research (pp.403-412). Thousand Oaks, CA: Sage.
Honigmann, John J. (1976). The personal approach in cultural anthropological research. Current Anthropology, 17(2), 243-261.
Knoblauch, Hubert; Baer, Alejandro; Laurier, Eric; Petschke, Sabine & Schnettler, Bernt (2008). Visual analysis. New developments in the interpretative analysis of video and photography. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 9(3), Art. 14, http://dx.doi.org/10.17169/fqs-9.3.1170 [Accessed: October 1, 2017].
Leather, Phil; Beale, Diane; Santos, Angeli; Watts, Janine & Lee, Laura (2003). Outcomes of environmental appraisal of different hospital waiting areas. Environment and Behavior, 35(6), 842-869.
Lefebvre, Henri (1991). The production of space. Oxford: Blackwell.
Levine, Robert (1987). Waiting is a power game. Psychology Today, 21(4), 24-33.
Low, Setha (2016). Spatializing culture: The ethnography of space and place. Abingdon: Routledge.
Milton, John (1991 [1655]). When I consider how my light is spent. Sonnet 19. In Stephen Orgel & Jonathan Goldberg (Eds.), John Milton (p.81). Oxford: Oxford University Press.
Mulcahy, Caitlin M.; Parry, Diana C. & Glover, Troy D. (2010). The "patient patient": The trauma of waiting and the power of resistance for people living with cancer. Qualitative Health Research, 20(8), 1062-1075.
Neuwelt, Pat M.; Kearns, Robin A. & Browne, Annette J. (2015). The place of receptionists in access to primary care: Challenges in the space between community and consultation. Social Science & Medicine, 133, 287-295.
Noesjirwan, Jennifer (1977). Contrasting cultural patterns of interpersonal closeness in doctors' waiting rooms in Sydney and Jakarta. Journal of Cross-Cultural Psychology, 8, 357-368.
Pauwels, Luc (2011). An integrated conceptual framework for visual social research. In Eric Margolis & Luc Pauwels (Eds.), The Sage handbook of visual research methods (pp.3-23). Thousand Oaks, CA: Sage.
Petersen, Nicoline J. & Østergaard, Sille (2003). Organisational photography as a research method: What, how and why. Copenhagen: CBS, http://www.aacorn.net/members_all/ostergaard_sille/organizationalphotography.pdf [Accessed: June 27, 2017].
Pink, Sarah (2007). Doing visual ethnography. London: Sage.
Rittenmeyer, Leslie; Huffman, Dolores & Godfrey, Chris (2014). The experience of patients, families, and/or significant others of waiting when engaging with the healthcare system: A systematic qualitative review. JBI Database Systematic Review Implement Reports, 12(8), 193-258.
Robson, Colin (2016). Real world research: A resource for social scientists and practitioner-researchers (4th ed.). Oxford: Blackwell.
Saumure, Kristie & Given, Lisa (2008). Convenience sample. In Lisa Given (Ed.), The Sage encyclopedia of qualitative research methods (pp.124-125). Thousand Oaks, CA: Sage.
Schwartz, Barry (1974). Waiting, exchange, and power: The distribution of time in social systems. American Journal of Sociology, 79(4), 841-870.
Schweizer, Harold (2005). On waiting. University of Toronto Quarterly, 74(3), 777-792.
Sime, Jonathan D. (1986). Creating places or designing spaces?. Journal of Environmental Psychology, 6(1), 49-63.
Street, Alice & Coleman, Simon (2012). Real and imagined spaces. Space and Culture, 15(1), 4-17.
Tallis, Raymond (2013). On waiting. Philosophy Now, 96, 48-49.
Tanner, Laura E. (2002). Bodies in waiting: Representations of medical waiting rooms in contemporary American fiction. American Literary History, 14(1), 115-130.
Tsai, Chun Yen; Wang, Mu-Chia; Liao, Wei-Tsen; Lu, Jui-Heng; Sun, Pi-Hung; Lin, Blossom Jen-Yu & Breen, Gerald-Mark (2007). Hospital outpatient perceptions of the physical environment of waiting areas: The role of patient characteristics on atmospherics in one academic medical center. BMC Health Services Research, 7:198, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2231355/pdf/1472-6963-7-198.pdf [Accessed: October 1, 2017].
Gary CLAPTON is a senior lecturer in social work, in the School of Social and Political Science at the University of Edinburgh in Scotland. He holds a PhD in social work from the University of Edinburgh (2000), a master in sociology and social policy from the University of North London (1993) and is a qualified social worker. His main research interests are within the field of fathers and families, adoption and moral panics. He is happily out of his comfort zone with this enquiry into waiting.
Contact:
Gary Clapton
Social Work, School of Social and Political Science
University of Edinburgh
Chrystal Macmillan Building
15a George Square
Edinburgh, EH8 9LD, UK
E-mail: gary.clapton@ed.ac.uk
Clapton, Gary (2018). The General Practice Health Waiting Area in Images: Threshold, Borderland, and Place of Transition in the Sense of Self [43 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 19(1), Art. 6, http://dx.doi.org/10.17169/fqs-19.1.2896.

Creative Commons Attribution 4.0 International License