Volume 24, No. 2, Art. 23 – May 2023
Personalized HIV Treatment: Bringing Marginalized Patients to the Forefront With Situational Analysis
Renate Baumgartner
Abstract: Since the early 2000s, personalized medicine (PM) has been a much-hyped field of healthcare. HIV treatment optimization tools were one of the first successful examples of PM, and have since their development been used to find tailored and optimized treatment for HIV-positive people. In this paper on a case study of the social arena of personalized HIV therapy I show how social worlds worked on both shared and distinct goals within the arena. I highlight the simultaneous centering and marginalization to which people seeking HIV therapy were subjected discursively in the social worlds. I also demonstrate that the further patients were from practitioners' daily work, the more they were reduced to their blood samples, rather than being constructed as complex and human.
Key words: personalized medicine; antiretroviral therapy; health care; artificial intelligence; machine learning; implicated actors
Table of Contents
1. Introduction
2. HIV Treatment Optimization Tools and the Arena of Personalized Medicine
2.1 The emergence of AIDS and the HIV
2.2 HIV/AIDS-treatment
3. Social Worlds, Social Arenas, Implicated Actors, and Discursive Constructions
4. Analysis
4.1 Social worlds in the arena of the researched ML-based HIV TOS development
4.2 Marginalized while centered actors ("patients")
4.3 Categorization schemes of patients in different social worlds
4.3.1 Categorization based on patient's therapy status
4.3.2 Categorization based on patient's compliance
4.3.3 Categorization based on social determinants of health
5. The Productivity of the Social World, Social Arena Framework for Analysis
6. Outlook
Since work in artificial intelligence (AI) was propelled forward by major advances ca. 2012, the technology has been framed as a remedy for current challenges in healthcare (TOPOL, 2019). Early examples of the involvement of AI, and more precisely machine learning (ML) in medicine can be found in personalized medicine (PM). Having been intensely hyped since the 2000s, different stakeholders were involved in PM and entered established arenas of healthcare, such as bioinformaticians and computer scientists (ERIKAINEN & CHAN, 2019). A commonly shared goal in healthcare was to ensure good health for patients. For a chronic infection such as HIV this goal is particularly ambitious. People with human immunodeficiency virus (HIV) were historically neglected by the medical community. Persistent efforts of HIV activists succeeded in influencing the research community, and the development of and access to essential medications was established (EPSTEIN, 1996). Today, HIV treatment is framed as a success story of medicine: While an HIV diagnosis was a virtual death sentence through infection only decades ago, nowadays, with the right choice and availability of, and compliance with antiretroviral therapy, most HIV-positive people have a similar lifespan to those without HIV (Deutsche AIDS-Gesellschaft e.V. [German AIDS Society] [DAIG], 2020a). [1]
Machine learning techniques were introduced to the field of HIV-1 antiretroviral therapy in the early 2000s to suggest tailored treatment options particularly for those for whom treatment selection was difficult. During the empirical research on these ML applications, I soon realized that the different stakeholders involved or standing at the sidelines of development interpreted the relevance of the tools very differently and expressed different goals while pursuing the development. Additionally, they constructed people with HIV seeking treatment in very different ways. The situational analysis (SA) framework will be shown to be well-suited for analyzing social worlds, groups who share commitment for activities, views, and/or goals which sometimes overlap with professional groups. With the help of SA, one can analyze how different social worlds interact in social arenas, where they work together on a shared problem and come to agreements about common goals. Within such arenas we also find people who are not organized in groups with shared activities, what Adele CLARKE and Susan Leigh STAR (2008, p.113) called "implicated actors." Inspired by feminist philosophy of science perspective, CLARKE, FRIESE and WASHBURN (2015) suggested that researchers focus particularly on marginalized actors who cannot influence how they are perceived or constructed by social worlds. Generally, the SA framework is firmly grounded in the sociology of science and technology. Both were used by researchers to analyze how technologies can change scientific research and healthcare and how this influences different parties, such as social worlds and the implicated actors involved (CLARKE, SHIM, MAMO, FOSKET & FISHMAN, 2003). [2]
In this paper I present the results of an exploratory study on the productiveness of the SA framework on personalized HIV therapy in Germany as a case study in PM. I applied the social worlds/arenas concept in my analysis of how work was done within and among different social worlds within the arena of personalized HIV therapy and of which goals and activities social worlds as collective actors shared. In the first part of the paper (Section 2), I introduce the arena of personalized HIV therapy, its emergence of which was a result of work on HIV, HIV infections, and antiretroviral therapy (BEERENWINKEL et al., 2002). In Section 4 I show how people seeking antiretroviral treatment were present as implicated actors in the arena and how practitioners in the social worlds constructed them discursively in different categorization schemes which are related to the work of the different social worlds. Finally, in Section 5 the productivity of the categorization schemes for the social worlds will be discussed, as their consequences for the implicated actors, who were simultaneously centered for the shared goal of the social worlds (ensuring patient survival) and marginalized in the world's social constructions. While considering nuanced processes of marginalization of actors/actants, the suitability of SA for researching PM and digital transformations by AI will be examined from a critical stance. [3]
2. HIV Treatment Optimization Tools and the Arena of Personalized Medicine
PM has since the early 2000s been a much-hyped field of medicine, with which scientists were able to attract considerable funding for biomedical research and healthcare. The most common goal within PM has been to use biological (mostly genetic) data to provide targeted treatment to individuals (PRAINSACK, 2017). Genetic and other data about patients and illnesses have been analyzed and interpreted with the help of algorithmic systems. More recently, the applications have also been based on ML or other forms of AI which include algorithms that are trained with data to which they are exposed specifically for the task for which they are used. Due to their focus on digital data and its analysis, the development and curation of the applications new collaborations between social worlds were established. The collaborative work of healthcare experts, physicians, biologists, bioinformaticians, and others has been necessary for developing, evaluating, and refining digital tools used for PM (ERIKAINEN & CHAN, 2019). While PM has been under critique for huge expenditures not leading to an equal number of useful tools for clinical routine, HIV treatment optimization tools (HIV TOS) are an example of a successful application of PM that has been in use for almost two decades (BAUMGARTNER, 2021a). [4]
The ML tools which I researched are part of a family of ML-based tools based on support vector machines (BEERENWINKEL et al., 2002). They were developed and have been used within the arena of PM with the aim of treatment optimization for people tested positive for HIV1). The tools have been used to screen RNA data from blood samples of HIV-1-positive people for resistances to available active antiretroviral ingredients. Developers of the tools also promised that the tools provide a prediction which antiretroviral drugs would be most effective against the specific HI viruses of individual patients. Due to this claim of tailored treatment the tool could be labelled as PM. The expansion of the existing social arena of HIV treatment to include the social worlds of bioinformaticians and computer scientists was a prerequisite for the development and use of these treatment optimization tools (TOS). Members of these social worlds are experts for the algorithmic reformulation of a task (e.g., to predict resistance from genetic data), and for the programming, maintenance, and servicing of the algorithmic system. [5]
2.1 The emergence of AIDS and the HIV
In 1981 the Centers for Disease Control and Prevention noted that a few young homosexual men suffered from a type of pneumonia and a rare form of skin cancer uncommon for young, healthy people. Soon, these diseases were attributed to the early patient's "lifestyle" (homosexual sex and promiscuity) and referred to in a homonegative way as the "homosexual plague" or the "gay disease," thereby stigmatizing homosexual and bisexual men and men having sex with men. At first there was no treatment available, and politicians of many countries (including REAGAN in the US, THATCHER in the UK, and GAUWEILER in Bavaria/Germany) were not interested in providing a treatment but rather in further marginalizing affected groups with high incidents of HIV/Acquired immune deficiency syndrome (AIDS), such as homosexual men, sex workers, and drug addicts. This resulted in HIV-positive individuals and whole communities (lesbian, gay, bisexual, and transgender [LGBT]) rising up in activism for research on and a suitable treatment for HIV/AIDS, and resisting their marginalization (BEISSWENGER & HÖPFNER, 1993). In 1982, the disease got its official name, AIDS, because it weakens or destroys the immune system and makes the body vulnerable for various types of infections. Shortly afterwards, as AIDS cases were reported in many countries and on all continents, AIDS was given the status of a world health problem, which it remains to this day (EPSTEIN, 1996). [6]
In 1983, the virus that causes AIDS was discovered and later named Human Immunodeficiency Virus. As a retrovirus, HIV's genetic information is contained on a single strand of RNA. The virus enters the cell, forcing it to transcribe the viral RNA into the cellular DNA. The cell then produces new viruses according to the rival HIV-RNA specifications. HIV primarily affects what are called CD4 lymphocytes/helper cells, which are essential for a functioning immune system. Every day, millions of new viruses are produced in the organism of an HIV-infected person, and just as many viruses are destroyed by the immune system through the destruction of helper lymphocytes. This can be compensated by the immune system for many years, but eventually the decrease in the helper lymphocytes weakens the body's own defense system. HIV reduces the body's ability to fight infections and disease and can then lead to death via opportunistic infections and tumors (GALLO & MONTAGNIER, 2003; SCHMID, 2018). In the late 1980s it was found that HIV is especially prone to mutate. This remains one of the major challenges in treating HIV infections (EPSTEIN, 1996). [7]
The first medication for HIV-infected people, called azidothymidine (AZT), only became available in 1987 and was at first used as a single drug treatment. Besides the severe side effects, the problem of this single drug treatment was that mutation-prone HI viruses developed drug resistant mutations. Once the virus is resistant to the drug, the treatment stops working and the immune system deteriorates, leading to the infections and tumors mentioned above (EPSTEIN, 1996). Over the following years, several other drugs similar to AZT were released. Initially, these were also administered as single drug treatments sequentially in response to the development of medication resistances. Soon, people treated in this way ran out of medication options. In the 1990s, a treatment approach was trialed where three or more drugs were given in combination, called highly active antiretroviral therapy (HAART). Only with the advent of HAART in the mid-1990s did long-term effectiveness of HIV/AIDS therapy become possible by pushing the viral load to a very low level. With this new form of therapy resistance-inducing mutations of the virus against available antiretroviral drugs could be stopped. HAART has prolonged the lives of many HIV-infected people and its widespread use has resulted in HIV being rather a chronic disease than a constant threat to life. Thus, the main goal of antiretroviral therapy to date is that viral load is decreased as much as possible, ideally to an undetectable level, which also diminishes the chances of HIV transmissions. Even then, HIV resides permanently in the body. Hence, antiretroviral therapy is to be taken lifelong and without interruption. Both therapy interruptions and underdosing of the medication carry a high risk of treatment failure due to the development of resistance (DAIG, 2020a). Therefore, a patient's compliance in regular and lifelong drug administration is required for a successful antiretroviral therapy. In the mid-2000s, single-tablet regimens were approved, in which HAART, consisting of several active ingredients, was combined in one daily tablet (EUROPEAN MEDICINES AGENCY, 2018 [2007]). This represented a breakthrough in HIV treatment for the physicians and patients involved, making it significantly easier to follow an active treatment regimen. Patients' compliance was better achieved with the simplified treatment regimen. This led to increased treatment success. Nevertheless, virologist Bio1 in my study reported there were around 10% HIV-positive patients for whom resistances complicate the choice of treatment (Bio1, r.282ff.2)). Here, different experts from different social worlds come into play, as we will see in the following analysis. [8]
3. Social Worlds, Social Arenas, Implicated Actors, and Discursive Constructions
The key focus of SA is "interpreting the situation per se" (CLARKE et al., 2018, p.27). Theories of William I. THOMAS, George H. MEAD, John DEWEY and especially Herbert BLUMER led to the concept that "a situation is a gestalt greater than the sum of its parts" (CLARKE et al., 2018, p.71). "This invisible agency of the situation per se" is "the momentum of the relationality among the different elements of the situation" (p.70) and is the key interest to be explored during analysis. The concept of social worlds has been used "since the early days of Chicago-style interactionism" (STRAUSS, 1978, p.119) and is "the conceptual infrastructure of situational analysis" (CLARKE & STAR, 2008, p.114). As "social wholes" (p.115) from the Chicago School of Sociology in the 1950s and 1960s, they were used to study work and professions focusing on shared discourses, instead of geographic boundaries, also considering the interaction and discourses between them. Within the modern version of social worlds theory, social worlds "generate shared perspectives" (ibid.) as a basis to work on shared activities and to "achieve their goals" (ibid.) with shared resources of various kinds (see also CLARKE et al., 2018, p.71; STRAUSS, 1978). Social worlds have at least one primary activity, specific sites, and involve technology to pursue their activity (CLARKE et al., 2018; STRAUSS, 1978). Social worlds are procedural, i.e., they do not exist by themselves, but only become visible in practical consequences: They come into being and exist only through the joint commitment of their members regarding their core activity and the mutual reference to each other. It is through engaging and participating in social worlds and arenas that individual and collective identity is formed (CLARKE & STAR, 2008). Especially for modern societies, it is constitutive that people belong to many different social worlds, i.e., have multiple memberships, which are susceptible to change. This creates overlaps at the edges of and differences between social worlds. Thus, social worlds intersect, segment into subworlds and are fluid (CLARKE et al., 2018; STRAUSS, 1978, 1984). "Social worlds are groups of varying sizes that generate life of their own" such as a discipline or a profession (CLARKE et al., 2018, p.71). In this perspective, "society as a whole can be conceptualized as consisting of a shifting mosaic of social worlds that both touch and interpenetrate" (CLARKE, 1998, p.16). Important characteristics of social worlds are MEAD's understandings of a shared perspective and commitment to a situation/arena. When social worlds grow and intersect into arenas, "their joint courses of commitment and (inter)action are articulated through discourses" (CLARKE & STAR, 2008, p.116). Following MEAD, one can conceptualize them as "universes of discourse." These discourses are "in collective, material action" (p.115). [9]
Social arenas are "composed of multiple worlds organized ecologically around issues of mutual concern and commitment to action" (p.113). From an analytical perspective, with the concept of social arenas one can analytically determine the processes of exchange and the relationships between social worlds and subworlds. It is a scalable concept, with which larger and smaller arenas can be investigated in and between social worlds (STRAUSS, 1993). Being part of Chicago School interactionism, social worlds/arenas theory also lends itself to the analysis of differences, e.g., of perspectives between social worlds. Anselm STRAUSS saw social worlds and arenas as "significant sites of negotiations" and "negotiating" as "major social process" (CLARKE et al., 2018, p.73). CLARKE et al. described arenas also as "discursive sites" that can last over time and will then be "characterized by multiple, complex, and layered discourses" (p.73). As "sites of contestation and controversy," arenas are a particularly helpful tool for analyzing "heterogenous perspectives, and position on key elements, and to see power in action" (p.73). Within CLARKE et al.'s framework, "work activities, organization, and discourses" (p.75). i.e., practices of and action within social worlds rather than individuals, are the focus of analysis. Further, both human and nonhuman elements of a broader situation can be considered and have agency. Working with different analytical maps is an essential feature of SA. Social worlds/arenas maps can be used to "lay out the collective actors, key nonhuman elements, and the arena(s) of commitment and discourse within which they are engaged in ongoing negotiations—[i.e.,] mesolevel interpretations of the situation" (CLARKE & STAR 2008, p.128). Since the 1980s, social worlds theory has also been used in STS and studies of social worlds in the life sciences, e.g., to explore nonhuman actors, tools and infrastructures (CLARKE & STAR 2008). [10]
From various studies with social worlds theory (many focused on scientific work practice), what BLUMER (1969) called "sensitizing concepts" (p.147) have been generated. According to him, these concepts are not clear definitions and specifications (definitive concepts), but rather suggest a direction for the investigation. CLARKE and STAR (2008, p.117) named a whole toolbox of sensitizing concepts that can be used for analysis in social worlds theory "to think about the relational ecologies of social worlds, arenas, and their discourses." One sensitizing concept which has a prominent place in situational analysis is that of implicated actors/actants. This concept was a result of CLARKE's empirical research (CLARKE & MONTINI, 1993) and can be a useful tool to analyze relative power in social worlds/ arenas: "It focuses on the situatedness of less powerful actors in a situation and the consequences of other's action for them, raising important issues of discursive constructions of actors and nonhuman actants and their consequences for those actors" (CLARKE et al., 2018, p.76). Implicated actors are constructed by others for their own purposes. CLARKE and STAR described "at least two kinds of implicated actors" (p.119) which are relevant for the study reported here: "those who are physically present but are generally silenced/ignored/made invisible by those in power in the social world or arena," and those who are "not physically present in a given social world but solely discursively constructed and discursively present; they are conceived, presented, and perhaps targeted by the work of the arena participants" (ibid.). Implicated actors play no active part in the creation of their representation within these social worlds or arenas, their perspective is not seen as relevant by the members of the social worlds, and they are not asked to participate in the arena (ibid.). CLARKE and STAR formulated the following analytical questions for implicated nonhuman actors: "who is discursively constructing what, how, and why?" (ibid.), which I will show are also productive when studying implicated human actors. In the current analysis, the concept is used as a starting point to develop a suitable version of implicated human actors for this particular case study. [11]
For a more detailed analysis within the social worlds, the concept of discursive constructions was used. This term was adopted by Angelika POFERL (2004), Rainer KELLER, Andreas HIRSELAND, Werner SCHNEIDER and Willy VIEHÖVER (2005) and is connected to Peter L. BERGER and Thomas LUCKMANN's sociology of knowledge (1969 [1966]) and Michel FOUCAULT's discourse (1974 [1971]) (see also BOSANČIĆ & KELLER, 2019). Similar to grounded theory methodology (GTM, STRAUSS & CORBIN, 1994) and SA, it is connected to pragmatism insofar as problems in societal action and thinking are considered starting points for discursivation of phenomena and materialities. Saša BOSANČIĆ and KELLER (2019) spoke about discourses as connected to the materialities of existences. They "produce hard facts" and "bring order" to the field (p.2). The focus on analysis of discursive constructions in the methods mentioned above resonates with the power-critical orientation CLARKE built into SA, where the discursive work which happens in social worlds is analyzed with a view toward revealing power asymmetries. [12]
The following section contains my analysis of the project of the ML tools mentioned in the beginning of the chapter, which I examined as an example of an arena of PM for HIV treatment in Germany. I aim to illustrate how SA can be used in the course of a research project to analyze social worlds and implicated actors within an arena, and how the concepts sensitize the view of the researcher. As CLARKE et al. noted, "SA itself builds on the genitivity of the situation through analysis" (2018, p.70). SA, rather than the more traditional social worlds/arenas analysis of the arena of PM for HIV treatment, was chosen because of two distinct characteristics. Firstly, with SA the researcher can focus their analysis also on nonhuman elements. Even if those are not central in this particular analysis, keeping nonhuman elements, such as the HI viruses, blood samples, or the ML tools in mind during analysis was very important. Secondly, through CLARKE et al.'s approach, one can consider that even if social worlds are sometimes represented by a few voices of their members, those still speak for the social world as a whole. Hence, the analysis is not one of individuals, but one of collective "work activities" and discursive constructions that members of these social worlds develop. [13]
I will also explore how doing different iterations of a social worlds/arenas map can sharpen the analyst's sensitivity to different aspects within the analysis. I will illustrate this by presenting my analysis of (shared) goals and activities, and categorization schemes that the social worlds of virologists, bioinformaticians and physicians are discursively constructing, while searching for a suitable treatment against HIV. The analysis is based on semi structured expert interviews according to Michael MEUSER and Ulrike NAGEL (2010) with one physician (Med1), two virologists (Bio1 and Bio2), and two bioinformaticians (DS6 and DS7). They were chosen as experts in their field (all) and because they had published about the researched ML-tool (all virologists and bioinformaticians). Apart from the physician, all the interviewees were closely involved in the development of these tools. The interviews were transcribed verbatim before being coded based on GTM. Several documents on HIV treatment, homepages of the researched tools and the related social worlds, publications by them and guidelines for HIV treatment were coded and used in the SA. Social worlds and their organizations, activities, technologies, and goals were identified following the guiding questions that are sketched out under Section 4.1. Messy situational maps, relational maps, social worlds/arenas maps and mind maps detailing processes within the arena were used in the analytical process. Social worlds/arenas maps were adapted for the work in this case study. [14]
4.1 Social worlds in the arena of the researched ML-based HIV TOS development
When identifying social worlds, one usually focuses on analyzing the following questions: Which primary activities take place? Where do they take place? Which technologies are used? Which organizations are involved? An overview of these aspects is shown in Figures 1 and 2 and the analysis below. The initiative for the development of the researched ML TOS for HIV came from the clinicians who worked with HIV patients (Bio2, r.62ff.). However, virologists and bioinformaticians were central actors in the development of these tools and worked very closely together, with clinicians as advisers (Bio2, r.80ff.).3)
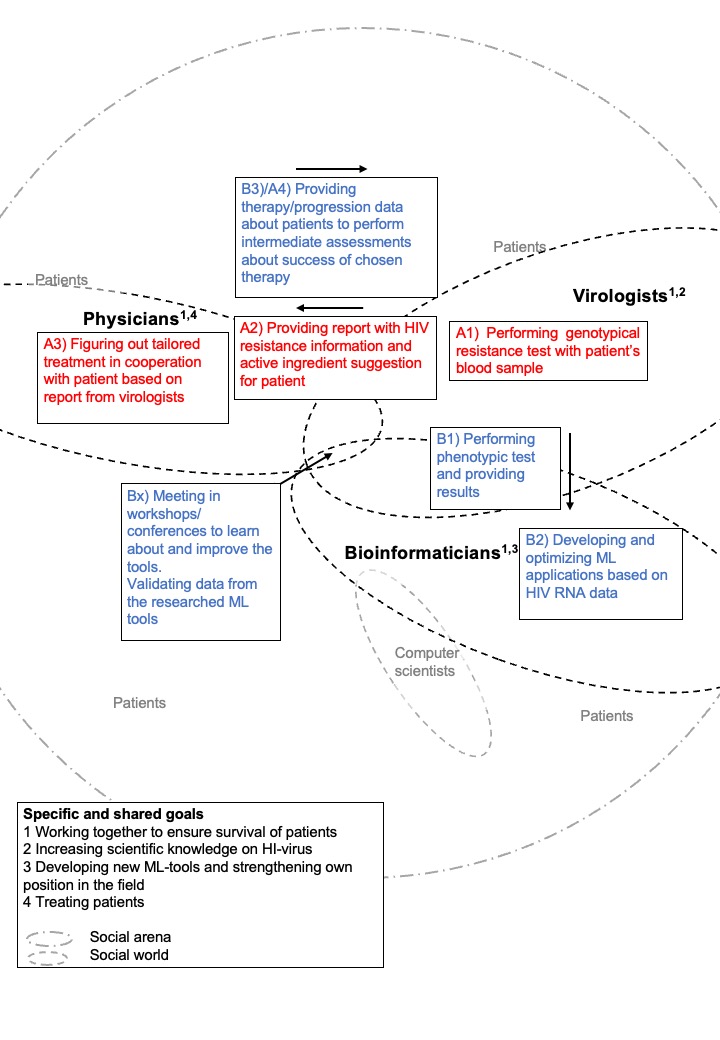
Figure 1: The goal and activities map of the researched ML-based HIV TOS. Please click here for an enlarged version of Figure 1. [15]
The primary activity of virologists Bio1 and Bio2 took place in laboratories at the University Clinic of Düsseldorf4) and consisted of sequencing the HI-viral RNA derived from the patient's blood sample to analyze the viral RNA for mutations and determine the presence of resistances. According to a literature search, two different sorts of tests can be used. The most common test was and still is the genotypical resistance test, which compares the HI-viral RNA with known other HIV, searching for mutations and predicting susceptibility of HIV to antiretroviral medication based on "interpretation systems"5) (Deutsche AIDS-Hilfe e.V., [DAH], 2010, n.P.; Gemeinsamer Bundesausschuss [G-BA], 2004, p.30). The second option is a phenotypical resistance test where the HI-viral RNA is checked in an in-vitro titration for existing resistances against known active antiretroviral ingredients. Different tests were carried out in different situations and different information was made available to different social worlds. Bio1 stated that virologists normally provide a report to the physician outlining the active antiretroviral ingredients to which the specific HIV is susceptible. The scientific basis of the report usually consists of results of genotypic resistance tests, which is the more economic option (DAH, 2010). Physicians used this to determine the most suitable antiretroviral therapy (Bio1, r.302ff.). Virologist Bio1 (r.78ff.) spoke about the advent of ML-based HIV TOS development. It started when they performed phenotypical resistance tests on the blood of therapy-failure patients. The resulting information—which HI virus was resistant to which ingredient—was the key training data for some of the earlier ML tools. Here the bioinformaticians, as experts in developing algorithmic applications for HIV TOS, came into play. Their primary activity, taking place mainly at the Munich Institute for Computer Science, was the development and optimization of ML applications based on the data the virologists obtained in the cell culture in the lab. This data was used as training data for the ML algorithms in the tools. Once the bioinformaticians and members of other involved social worlds were satisfied with the performance of the ML system, the application was released and freely available for everyone to enter HI-viral RNA sequences and obtain predictions of resistances regarding the specific RNA entered (DS6, r.1370ff.). While developing the researched ML tools, bioinformaticians had to coordinate their work closely with the virologists who are the experts on the virus, e.g., they needed to negotiate common definitions what "therapy-failure" means and how that could be translated to the algorithmic system (Bio1, r.446ff.). The bioinformatician recognized that to increase acceptance and the use of the tools, it was crucial for users (virologists and medical professionals) to understand how the tools worked, how the results are obtained, and how to use them properly6). The interviewed virologists, being expert users, usually evaluated the suggestion of the tools with their own scientific experience or scientific literature on the subject. The bioinformaticians also recognized that the tools must be adapted to the expectations and needs of the users (the community), before collaboration partners could be won (DS6, r.720ff.). Yearly workshops and conferences were organized for an exchange between different social worlds. In these arenas, physicians, virologists, and bioinformaticians gathered in person to discuss the tools more thoroughly, get feedback for further optimizations and developments, and exchange knowledge about functioning and correct use of the tools (DS6, r.456ff.). The attendees used these workshops to scientifically validate the outcome of the researched tools by discussing specific patient cases. [16]
The shared goal that connected the social worlds can best be described with the words of an interviewed virologist: "Ultimately, we want to ensure the survival of the patient [...] There should be a quality of life, right? And these- these are challenges where we have to have the courage to consider things that are not yet mainstream" (Bio2, r.366ff.). This means that actors in the medical field, biology, and bioinformatics worked together for the medical goal of ensuring survival of patients (Figure 2). One way this was achieved was by strategically linking existing knowledge from different research areas, and recruiting new stakeholders—in this case bioinformaticians—in order to be able to develop the ML tools. Further social-world-specific goals were to gain knowledge about virological diseases (virologists), to develop new algorithmic applications for use in other medical areas, e.g., cancer research and infectious diseases. This latter goal was mostly interesting for bioinformaticians, who aimed to apply their algorithmic systems in various medical areas (DS6, r.98ff.). In my analysis, I also identified the personal and/or professional goals of building a scientific reputation (all researchers). [17]
Despite the impression of concerted cooperation in the pursuance of common goals described above, reception of the researched tool was not universally enthusiastic. Its relevance was evaluated very differently by members of various social worlds. While the virologist and the bioinformatician saw a relevance in the tools they invented, the physician I interviewed (Med1), who was not part of the development, was not acquainted with the tools.7) Med1 understood their own role as consisting in working with the patient and finding a suitable therapy together, and acknowledged that expert knowledge regarding HIV would come from the virologists (the main users of HIV TOS). Med1 (r.1311ff.) did not identify any problems in finding a suitable and active therapy, even less so since single-tablet regimens became available. In summary, I have used the SA framework to demonstrate how applications based on AI and ML, such as the researched tool in the field of PM, were constructed within and through arenas composed of heterogeneous actors committed to action on a core issue. I have also shown that while commitment to common goals is characteristic of the work done in social worlds, individual actors experienced different levels of commitment. [18]
4.2 Marginalized while centered actors ("patients")
People with HIV who seek treatment were the connecting elements between the interviews, which makes sense considering the shared goal of the arena was to ensure their survival. The actors in the social worlds centered this group of people through this goal as pivotal actors within the arena. The existence of the patients has been a prerequisite for the existence of the arena. As implicated actors, the "patients"8) were present in diverse ways (Figure 2) and discursively constructed by actors in all examined social worlds (physician, virologists, bioinformaticians). However, the ways in which they were discursively constructed shows they were objectified and marginalized, which manifested as nuanced processes across social worlds. Two examples of this marginalization were being excluded from shaping the discourses about their own group and from being part of a decision that is above the level of their individual treatment.9) Thus, the patients found themselves in a position of less power compared to the actors in the social worlds within the arena.
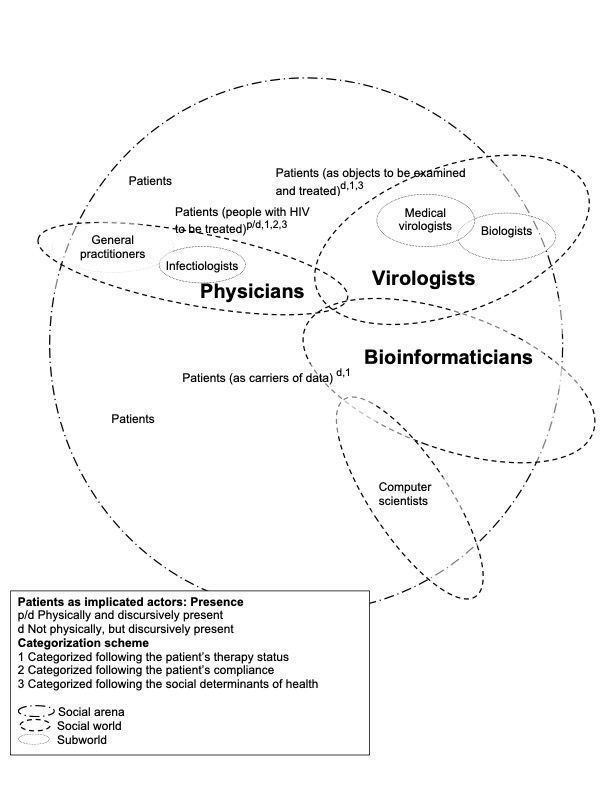
Figure 2: The arena of personalized HIV therapy. Please click here for an enlarged version of Figure 2. [19]
It was in the interview with the physician (Med1), who had the most real-life contact with people seeking HIV assessment or treatment, that the patients seemed most present as individuals. Physician Med1 specifically referred to compliance, stigmatization, pregnancy, and the patient's cultural background. For the physician, who saw people with HIV during regular control examinations, the patients were present physically and discursively, while technical applications played almost no role. Conversely, bioinformaticians had no physical contact with people with HIV but saw them in terms of their data. Bioinformatician DS6 discursively constructed them as carriers of data:
"So that means, when you now have a patient, normally you have one sequence per patient, right? With Sanger10) you have this one particular consensus sequence that you see. And with NGS you have several sequences per patient. Because you look deeper and see different virus variants" (DS6, r.632ff.). [20]
Seeing patients primarily in terms of their viral sequences, the professional group of bioinformaticians was the furthest away from people with HIV among the social worlds, followed by the virologists (Bio1 and Bio2). With the interviewed virologists, a more differentiated picture emerged. While Bio1 talked about people who had come for HIV assessment or treatment mainly in terms of the objects to be examined (i.e., blood samples which were subjected to resistance measuring), Bio2 presented a more holistic view on the disease, using references to popular culture and well-known personalities. When referring to clinical patients or those infected with HIV, they especially discussed people in terms of their cultural background, gender, e.g., as women and as pregnant women, and acknowledged their stigmatization, picking up similar topics as the physician. [21]
4.3 Categorization schemes of patients in different social worlds
In all examined social worlds, I could distinguish between different categorization11) schemes used to cluster patients into types. Members of each social world, depending on the internal logic that had been developed/negotiated, used certain categorization schemes fully and others just partially or not at all. The first categorization scheme related to the therapy status, the second one to the patient's compliance. A third scheme was based on social determinants of health that were made relevant for HIV-positive people (pregnancy, cultural background). [22]
4.3.1 Categorization based on patient's therapy status
Categorization based on the patient's therapy status was strongly prevalent in the accounts of the virologists, who regarded people with HIV as objects of treatment. Resistance tests were carried out at the beginning of treatment, when the viral load increased, and in the context of changing therapy. These tests provided essential information for the choice of the optimal antiretroviral therapy.
"That means we have these three cases: We have the therapy-naive, we have the failures whose viral load goes up, and we have those who do not have a viral load but want to change the therapy, for whatever reason. Those are the three cases" (Bio1, r.445ff.). [23]
Therapy-naive-patients: If a person's HIV test was positive, a resistance test was carried out in a virological lab using the person's blood sample. At this point the whole range of medication was still available for treatment in most cases; only about 10% of the therapy-naive-patients were infected with HI viruses that were already resistant to some drugs (so-called transferred resistances). The virologists examined the HIV in the blood and informed the physician about which active substances the virus is not resistant to. A therapy suggestion was made by the physician to the patient. The physician was the only one of the three expert groups who knew about a possible co-medication and other characteristics of the patient to be considered. The ultimate therapy decision was taken by the physician together with the patient. [24]
Therapy-failure-patients12) or the problematic/difficult case: According to my interviewees and in accordance with the Austrian-German guideline for antiretroviral therapy of HIV-1 infection (DAIG, 2020a), the viral load and the number of CD4 cells in the blood of HIV-positive people was measured every three to six months (the frequency depending on compliance, as assessed by the physician). As soon as the viral load increased, a resistance test was carried out. One reason for therapy failure could be virus mutations leading to resistance to the current drug therapy. Patient non-compliance was considered the main reason for this, i.e., "because the drug wasn't taken properly. That is the classic case. If the dosage isn't right, if it's underdosed, then the virus has a chance to replicate, to multiply, and that's when the mutations come about" (Bio1, r.202ff.). The virologists referred to these as "therapy-failure-patients," while the physician said, "the patient had a virological failure" or called them "problematic cases," and one bioinformatician spoke about "difficult cases" (Bio1, r.79; Med1, r.1104, r.419; DS6 r.1197). Asked for other possible explanations for the development of resistance, bioinformatician DS6 (r.1093ff.) replied: "That depends on many factors, so it can be that the medication is not taken regularly, or that the other medications had side effects, or that they had a gastrointestinal illness and therefore did not absorb the medication well." The physician and the virologists pointed out that it is usually older patients who had been in antiretroviral treatment for many years who experience therapy failure. A lack of effective treatment regimens over the course of decades meant many active ingredients had been tried out (also as single treatments), allowing a person's virus to develop resistances against many of the ingredients. This meant that ultimately, few active ingredients remained available to them, and it was difficult to offer a functioning HAART. However, at "maybe 1%" (Med1, r.400ff.), those cases were extremely rare. [25]
Change-of-therapy-patients: A third category consisted of patients whose therapy was being changed without having experienced a therapy failure. This was happening either at their own request due to co-medication, side effects, or drug interactions, or because simpler therapy regimens, e.g., single-tablet therapies, were available. In this case, there was no increase in the viral load, but a preventive check was carried out to determine whether there was any resistance to the drug under consideration. [26]
This categorization scheme was based on the logics of the social worlds13) that were invested in treating the chronic disease of HIV-positive people and ensuring their survival. Categorization into the patient types introduced above was most relevant for the work of virologists, and the full scheme was constructed by them and the physician (though one of the virologists and the physician did this descriptively and not in the exact terms I have used here). By categorizing patients into types, different practices and actions were triggered. The scheme also illustrates how the virologists saw patients as subjects in different treatment status groups. Since its approval in 2007, and with an increasing choice of different marketed variants within the last 5 years (Med1, r.192ff.), the single tablet remained the regimen of choice for most people treated for HIV infections in Germany. With this regimen good outcomes, i.e., low viral loads, could be obtained. This left only approximately 10% of patients that represented somewhat of a challenge for this social arena of PM, and 1% who represented truly difficult cases. This patient type seemed to be the most labor intensive one, mentioned by Bio1 as posing a particular challenge to their expertise. A "therapy-failure" was the type where members of all social worlds came into play, and it tied them together more strongly, uniting them in a need to rise to the challenge and collaborate to find a suitable therapy. This was also the only type of patient that was constructed discursively by all three social worlds, despite with slightly different meanings. While the virologists spoke of "failures," the physician and the bioinformatician spoke less judgmentally about "problematic" or "difficult cases," respectively (Bio1, r.445; Med1, r.1104, r.419; DS6 r.1197). These 1% of patients who had had a long history of therapy and who had already developed many resistances were the most demanding cases not only for virologists but also for bioinformaticians. The bioinformatician speculated that especially in such cases, the ML application could deliver better (or at least equally good) results compared to older rule-based systems (DS06, r.1202ff.). Ensuring the survival of this type of patient seemed therefore to be the main jointly constructed reason for the (ongoing) development of the researched family of ML tools. [27]
4.3.2 Categorization based on patient's compliance
The second categorization scheme reflected patients' compliance with their treatment regimen. It followed mostly the logic of the physician but was discussed by all three social worlds. Patient compliance was considered to be the decisive factor for therapeutic success. Since HIV therapy is life-long, durable patient compliance was and still is crucial. The physician constructed patients in this categorization scheme in terms of compliance-types:
"For some this is totally unproblematic, and it helps because they say: Yes, well, I'm home at seven every evening anyway, then I know I have my tablet. And for others this is very problematic. Then you have to make sure that you rather take something that has a higher threshold for developing resistance—I mean, when someone has a very, very irregular lifestyle. There really are some people who just party a lot and are out all weekend and so you just have to talk to people and see how reliably they can take the medication, to think together with them: What are the times in the day that you can keep, simply because compliance is infinitely important in HIV therapy" (Med1, r.202ff.). [28]
The categorization of the interviewed physician conformed to the categorization of the DAH, an umbrella organization of regional AIDS groups in Germany, which also differentiated between four types of patient compliance. They emphasized that "this categorization is of course quite rough and must be seen absolutely neutral, i.e., everyone is who they are, and no one is better than the other. However, this rough categorization helps the doctor to choose the right HIV therapy" (DAH, 2005, p.10). The implications of understanding patients in terms of belonging to different compliance categories were that physicians may choose a different form of therapy in dialogue with the patient depending on the anticipated compliance. Some treatment regimens must be taken reliably and precisely because missing out on pills would immediately decrease the effectiveness of the medication. Other therapy combinations are less sensitive in this regard and would still function if a dose is missed. The following categorization was published by the DAH (2005):
The normal type: Is not 100% perfect but trying to take their medication regularly. They almost always succeed in doing this, with a few exceptions that are within the framework of normal human forgetfulness and indisposition. A few tools are usually sufficient to reduce the "normal" forgetfulness. This is the desired compliance-type.
The holiday type: Usually take their medication reliably but not during vacation or at certain times of the year.
The party type: Like to be on the go and may not have their medication with them and then skip one or two whole daily doses.
The chaos type: Have no fixed daily routine and take their medication more or less regularly, depending on mood or external circumstances. [29]
Compliance was assumed to depend on the lifestyle of the patient, their attitude to therapy, the frequency of medication intake and the side effects or interactions of the medication. Furthermore, the social environment was considered to play an important role (stigmatization or acceptance), as well as the doctor-patient relationship, the professional competence of the doctor, and the atmosphere and organization in the practice/clinic. Since taking the medication was largely beyond the control of a physician as this happened as part of the patient's daily routine, the practitioner had to be able to rely on the patient's statements: "And others are adamant that they really take everything every day and they get resistances where you just don't know—are they actually taking it that way, or are there other problems?" (Med1, r.271ff.). Compliance could not and should not be achieved through coercion and pressure (Bio2, r.147ff.). Rather, the patient had to be fully informed. The doctor-patient relationship was of crucial importance here. The patients had to be able to articulate their needs and wishes:
"We do these analyses and try to find the safest possible combination of therapy for the patient. That is our concern, our job as virologists. And then the doctor's job—a doctor once said to me, 'Listen, have you ever considered that on the other end of that virus is a patient?' So, the patient has to want it, and do their part. And in the end, he has to take the medication—take it reliably. So, it's not enough to simply tell the patient, so, here's your prescription, bye. You have to get them to be invested" (Bio2, r.147ff.). [30]
Recruiting patients to participating in their own care was an essential part of the job of the physicians, but it was not always simply a matter of encouraging compliance with a drug regimen. For example, while some HIV patients were characterized as "willing to take risks" and try out new therapies (Bio2, r.242ff.), some older patients were described as sticking to old treatment regimens out of habit or fear of changing something that works, despite simpler, e.g., single tablet regiments being available (Med1, r.469ff.). It was also lamented that many patients had lost their fear of the disease because HIV can now be treated well and has "lost its terror" (Bio2, r.47ff.). [31]
In terms of good chances for therapy compliance, the single daily intake was regarded as the best available solution at the current time, even though long-acting implants were discussed by some of the interviewees. Compliance was conceptualized as the patient's submission to a specific daily routine: the necessity of eating at the same time every day and of taking responsibility for their own health through taking their medication regularly. This illustrates starkly that the role and responsibility attributed to patients was that they should do everything within their power to stay as healthy as possible. [32]
The great importance of compliance also made patients powerful. In the end, therapy success was not only dependent on the choice and availability of the right (or tailored) therapy but crucially on patients reliably taking their medication. The members of the social worlds whom I interviewed anticipated that without the cooperation of the person with HIV, the therapy would not work. This implies a transfer of responsibility to the patients which was accompanied by morally charged discourses within the social worlds. For example, questions of patients' trustworthiness were raised, especially by the physician. Interestingly, there were situations where the logic of the field was disrupted. Physician Med1 (r.252ff.) spoke about a long-term patient who only later in the therapy confessed that for years they had only taken part of their medication. Still, the measurement of the viral load did not show a decline in therapy success, almost as if the medication had been taken as intended. Examples like this could function as disruptions in the social worlds and members then questioned their internal logic. This led to a recognition of the patient as a "black box" (Med1, r.268ff.) and to hypothesizing over which other medical reasons could lead to this unexpected outcome, such as metabolism. [33]
Strikingly, though compliance was considered to be of paramount importance, the researched ML tools did not take this into account. At the core of the technology, resistance was conceptualized as being purely dependent on biological factors, while social factors, though constructed discursively as essential, were not included into the technology. This means that the assessment of the tailored therapy was always a multi-step process: viral properties were calculated by the technology and social features were taken into account by human experts (the physicians). [34]
4.3.3 Categorization based on social determinants of health
Besides age, which was made relevant as feature of long-term HAART, being biologically female and in the reproductive age was a category raised by the physician and the virologists. This coincided with the guidelines outlining that from a clinical viewpoint, pregnancy is a special condition of an HIV infection and a specific antiretroviral treatment was prescribed (DAIG, 2020b). The desire to have children should be made transparent to the physician to avoid clinical complications. Virologist Bio2 described how research has not come far enough regarding antiretroviral therapy for pregnant women. According to HIV therapy guidelines, some active ingredients were either contraindicated or were not yet approved for pregnant patients due to a lack of information regarding potential teratogenic effects of the active ingredients. This made the range of therapy choices for pregnant people more narrow (DAIG, 2020a). The guidelines also recommended HIV tests at the beginning of all pregnancies to minimize the risk of newborn infection. Especially before giving birth, and later during lactation, the viral load should be low to avoid infecting the newborn (DAIG, 2020b). Physician Med1 and bioinformatician Bio2 (r.316ff.) made the category pregnancy relevant mostly at the intersection of "the migrant woman." This might be the case because, as Med1 (r.680ff.) stated, "German women" who tested positive for HIV were in the minority. [35]
The category of migration background14), especially regarding people of African descent, was made relevant by the physician and the virologists. The interviewees mentioned that patients' cultural backgrounds played a major role, as there were different understandings of values and living conditions. While the "enlightened" German patient (Bio2, r.334ff.) was said to be able to communicate with the practitioner without language barriers and could read and understand package inserts for medication, for the migrant women a "patient self-help project" was organized (Med1, r.54ff.). Within this project for HIV-positive people (mostly women) of African descent, expert patients were organized to function as translators during physician-patient visits and as general buddies/mentors about HIV. Migrant women were also more often than non-migrant women described as poor or as single parents with many kids (Med1, r.746ff.). Bio2 (r.160ff.) and the physician said that patients from other cultures, especially women from Africa, sometimes had different values, e.g., regarding childbirth and breastfeeding, and lifestyle habits, e.g., stronger roots in their own community, which were sometimes a source of conflict between patient and practitioner. In addition, Med1 and Bio2 spoke about communication problems that have an impact on compliance. Some of these factors were given as justification for establishing the patient self-help project (Med1, r.71ff.). [36]
The way members of social worlds in this arena constructed this specific category at multiple intersections (migrant + woman + single mother + low income) could be regarded as special engagement and cultural sensitivity but also as othering or racist. Another reason given for the organization of the patient self-help project for HIV-positive people was what was described as the very common practice of gossiping within these communities.15) This, it was observed, would discourage people from sharing their HIV status in the presence of a typical translator and they often felt safer with an expert patient translating for them (Med1, r.71ff.). From epidemiological studies it is known that for a long time, migration background was correlated with HIV infection (Robert Koch-Institut [Robert Koch-Institute], (RKI), 2021). Now on the decline, people coming from Sub-Saharan Africa to Germany constituted a large proportion of people given initial HIV diagnoses in Germany between 2004 and 2021 (p.7). The categories of men having sex with men and intravenous drug users, which were also present in the epidemiological study by the Robert Koch-Institute, were only indirectly addressed by the different interviewees. [37]
In general, the categorization schemes seemed to be discursively constructed by members of the social worlds to create a simplified typology. These discourses were related to phenomena and materialities, and were used to "bring order" and "produce hard facts" ensuring an ability to act (BOSANČIĆ & KELLER, 2019, p.2). The importance of these orders can also be explained along the lines of Joan H. FUJIMURA's (1987, p.257) framework, within which she aimed to conceptualize scientists' efforts to construct "doable problems." Doability was usually obtained through "the alignment of three levels of work organization: experiment, laboratory, and social world" (p.261). Scientists achieved alignment by articulating—considering, collecting, coordinating, and integrating—tasks between these levels of work organizations (FUJIMURA, 1987). In my example, categorization schemes were important for the members of the social worlds in negotiating common understandings within and between the different social worlds and for being able to act in coordination to reach shared goals. [38]
5. The Productivity of the Social World, Social Arena Framework for Analysis
The social world/arena framework could be used in many productive ways for this case study. First, with the help of the framework I showed who constitutes a social world, how social worlds are connected or not, which activities and goals are specific for a particular social world, and which ones they share. The social worlds/arenas map as the central tool of the analysis can also be adapted to the needs of the study. In this project, two iterations of the social worlds/arenas maps proved especially helpful. The map in Figure 2 depicts the social worlds and those actors not organized in social worlds as well as the way they are present between social worlds and in which categorization scheme they are discursively constructed. In the map in Figure 1 activities as well as specific and shared goals of the social worlds within the arena are depicted. Physicians and virologists worked together to find a suitable antiretroviral therapy and virologists and bioinformaticians, together with some physicians, shared in the development of the ML-based HIV TOS. In the two maps, I show how patients were simultaneously centered through the shared goal of the social worlds and marginalized in the way they were discursively constructed. [39]
The analysis of specific and shared goals was important for the understanding of the longevity and success of the project and for a better understanding of the position of the patients especially in relation to their discursive construction by members of the social worlds in this arena. The specific shared goal in this arena was working together to ensure the survival of patients. Virologists were also interested in their scientific pursuit to understand the HI virus and bioinformaticians were invested in trying out their ML methods to optimize them and apply them to other (more promising) fields, e.g., cancer. The physician saw their role as treating patients. Under the umbrella goal of ensuring the survival of patients, the professions could pursue their own distinct aims. The specific and collective goals were based on the known reasoning within PM that more precise data gathered through/processed with algorithmic means were the link to a better understanding of a disease. In the end, the goal was to identify an optimized and individualized treatment, which it was thought would ensure the (longest) survival of patients. [40]
Connecting the interviewees' goals to their views on the patients I can show that they mostly followed a logic accordant with their profession. For the bioinformaticians, patients were constructed as data because they needed data to optimize their tools. For the virologists, the virological information of the patients and their reaction to the treatment was key, as this shows how suitable the active ingredient suggestion based on resistance testing was. Physicians constructed the patients as people with HIV to be treated. In fact, people with HIV were simultaneously made beneficiary of the common goal and subject to the distinct goals of social worlds; though the practitioners in all the social worlds declared unanimously that their primary aim was to ensure patients' survival, it was clear that for members of two social worlds central to this arena, their own agenda was no less important. [41]
A feminist theory of science was foundational for CLARKE et al. (2015; see also OFFENBERGER, 2019). Accordingly, she and her co-authors were particularly interested in identifying those who are at the margins of a social arena or who are marginalized by others. Individuals in an arena who are not connected with others in a similar situation—in analytical terms, organized in a social world—are more vulnerable. This can especially be true for the arena of healthcare. Using the framework, I have shown how HIV-positive people within the arena of HIV treatment were categorized by members of different social worlds. As has been established above, they were simultaneously central to the arena and marginalized because they were rarely constructed as actors acting in their own right. HIV-positive people seemed to be involved in the choice of their own treatment, but not in the optimization of the decision-making process or in the basic questions of whether further development of such tools was the right approach or of which other projects might be more beneficial for different patients.16) One could say the categorization just followed the logic of the field and has no moral account. However, this can also be analyzed from a power-critical perspective. Virologists referring to and constructing people as "therapy failure" or "failure" raised the question of in which contexts members of the social world used these terms and in the presence of whom (Bio1, r.79, 446). What is the effect on the work of social worlds when their members construct people as failures? Which effects do discursive constructions have on the responsibilization of the patients and moralization of their behavior and compliance? In my analysis of these discursive constructions, I revealed the interests and value systems underpinning the way people with HIV are characterized and the nuances of marginalization which are evident across the social worlds. The question is whether people treated for HIV are benefiting enough, even when the goals of the other social worlds, i.e., learning more about the virus or optimizing a ML-based tool, are at the forefront. [42]
I also demonstrated (Figure 2) that the physical presence of the implicated actors indeed changed how social worlds discursively construct them. The closer the members of a social world were to the patients, i.e., the more present physically people with HIV were with the practitioner, the more they were constructed by the practitioner as complex and human. This became apparent for example with the physician speaking at length about the influence of social determinants of health and emphasizing the need to decide on the treatment together with the patients. Physicians constructed the patients with different features: gender, ethnic background, age, and compliance type, which is connected to a type of lifestyle. These are general categories of people usually used within Western societies when referring to individuals as humans. However, the physician did not only refer to patients as humans but also constructed humans as patients in terms of compliance, entailing a specific role in this context where people are expected to adhere to specific activities to be considered worthy of help or are objects of examination. The virologists constructed HIV-positive people as objects to be examined with regard to resistant HI viruses and treated for them. Being experts for the viral part of HIV and its resistances, virologists were mostly interested in the outcome of the therapy. In the logic of this social world, the categorization of patients' therapy status was the most relevant one, because it was action-guiding. A "therapy-naive" person had still many choices for therapy, a "change-of therapy-patient" had to be checked for their treatment history (Bio1, r.446ff.). The occurrence of a "therapy-failure-patient" was the time when virologists could prove their skills to members of the other social worlds in the arena (Bio1, r.79). Work on these difficult cases also united actors in the arena in striving toward their shared goal of ensuring patient survival. Virologists—and the bioinformatician even more so—constructed patients predominantly as objects detached from their humanness: They were reduced to samples to be examined for resistant HI viruses and treated against HIV for the virologists and to carriers of data for the bioinformatician. It seemed that especially for the bioinformaticians, social determinants of health were not relevant. [43]
In the arena of personalized HIV treatment, it was possible to rank the discursive constructions of HIV-positive people used by members of the social worlds from more human to more objectified in the order physicians, virologists, bioinformaticians. This coincides with the closeness of practitioners in the field to the patients. The less members of a social world centered people as humans within their work, the more objectifying the discursive construction of people with HIV was. It is important, however, that commonness not breed complacency, because the consequences of this objectification can be grave for people seeking treatment for HIV: As practitioners in the fields of medicine and healthcare embrace more data-driven applications such as PM, patients' risk being inadequately understood as complex and human, which, in the worst case, can compromise their care. Patients might be reduced to their data points and dehumanized. This can represent an even bigger problem for marginalized people, whose discrimination stemming from systemic inequalities might then be dismissed as individual problems (BAUMGARTNER, 2021a; PRAINSACK, 2017). [44]
In this case study, the physicians who were closest to the patients did not work directly with the tools. Virologists and bioinformaticians developed the ML tool, the virologists used the tool and conveyed the outcome to the physicians. The physicians then decided on the suitable antiretroviral medication together with the patient. They only provided the information about the therapy outcome back to the virologists, so the virologists could validate their assessments and the quality of the tool's outcome, similar to a feedback loop. It is difficult to retrospectively analyze how the introduction of algorithmic HIV TOS might have changed the way treated people were conceived of by practitioners in the field of HIV treatment. One could surmise that the way of constructing patients as carriers of data—a construction introduced by the bioinformaticians with the beginning of ML-based HIV TOS—would circulate in the whole arena. However, at least the interviewed physician, who was not part of the development, did not construct their patients this way (while at the same time speaking of other ML-based applications and presenting knowledge about the importance of patient data for these). This point would have to be explored with physicians who were part of the development in order to understand whether more involvement with PM changes the way they discursively construct patients. [45]
Through the analysis we can also see how closely members of different worlds aligned in their understanding of the patients. In my case study, some parts of the categorization schemes were present throughout the social worlds (e.g., "therapy failures"), while categorization based on social determinants of health were shared by physicians and virologists, and the categorization scheme based on compliance types and lifestyles was used only by the physician. Shared discursive constructions might be interpreted as closer relationships between actors in social worlds because a shared understanding and ways of thinking about certain subjects might be indicated through them. A categorization scheme used by just one social world could mean that its logic is only relevant for this very social world, such as thinking in lifestyle categories to anticipate compliance was mostly relevant for physicians, who based their decision on the tailored therapy on this assessment. Interestingly, this important information was not adopted by bioinformaticians, who could have introduced it in their tool. This hints at the way HIV infection was constructed for the work in different social worlds. Seemingly, bioinformaticians above all constructed it as a purely biological disease, not conceptualizing it as also being influenced by social factors. The question is whether this way of thinking migrates through the ML tool back to the users of the tool (in this case virologists and not physicians). [46]
In this explorative study I show how productive SA can be when analyzing social worlds, arenas, and implicated actors. The framework is suitable for researching case studies of digitization in medicine and healthcare such as PM and introduction of AI in different fields. The social worlds/arenas maps were also used to depict different points of time within the arena, e.g., pre-AI introduction and post AI-introduction. With its strong focus on analyzing power asymmetries and focusing on marginalized actors/actants, SA is particularly suitable for a critical analysis of newly introduced AI in different fields. SA researchers can flesh out complexities in the social arenas during analysis. Tinkering with and adapting social worlds/arenas maps fosters the creative process and the development of an understanding of the analyzed situation. With SA, researchers can distinguish between specific and shared goals and their influence on members of social worlds as well as on actors in the arena who are not collectively organized. Researchers can also analyze logics and discursive constructions within different social worlds and make sense of similarities and differences between the worlds. The analysis reported here led me to important findings, such as the correlation between the degree of closeness of implicated actors to members of social worlds and the respective construction of those implicated actors as more/less complex and human. Through my mapping, I was able to show that centering actors in the arena does not prevent the same actors from being marginalized, as seen in the various discursive constructions discussed above. Thus, with the help of SA framework, marginalization could be conceptualized as a nuanced process that can be analyzed as it happens across social worlds. [47]
From the current study it is evident that people treated against HIV, despite being at the center of the arena—literally giving the arena of concern its raison d'être, were simultaneously implicated by others and marginalized. Members of professional groups whose specific professional goals are foregrounded in the arena should take care that this does not result in neglect of patients' needs. The umbrella goal of ensuring survival of the patients would have to be made more concrete and filled with patients' perspectives in addition to the specific goals of the social worlds involved so far: What do HIV-positive people need nowadays? How might already existing support groups, such as DAH, participate in representing and formulating those needs during the higher-level decision-making processes regarding suitable therapies and within the development of new tools? Currently, with single tablet regimens the survival of most HIV-positive people can be ensured without complications. Is the development of new and more precise, e.g., NGS-based HIV TOS, which might increase digitization and a deeper analysis of patient data, the right way to go? Or might other activities which put patients' health(care) needs at the center be more beneficial for the health and wellbeing of HIV-positive people? I advocate for participatory projects which include all stakeholders and a diversity of HIV-positive people, to collectively approach the question of which HIV TOS developments should be pursued. [48]
I would like to thank Darja BURLJAEV for her help in early stages of the paper and Tamara SCHWERTEL and two anonymous reviewers for their insightful feedback on the paper, as well as Sarah B. EVANS-JORDAN, Ursula OFFENBERGER, Birte KIMMERLE and participants of the working conference (especially Marc BUBECK and Bianca JANSKY) and members of the Tübinger SA interpretation group for their comments on earlier versions of this manuscript. I also thank Aljosha Victor KANNEWURF, Fanni WEBER and Sebastian BARTELHEIM for assistance in editing and proofreading the article.
1) There are also ML tools for HIV-2, hepatitis B, and hepatitis C, developed by the same group of people. However, those are not part of this analysis. The researched ML tool for HIV-1 was the first of the developed applications. <back>
2) With the numbers the lines in the transcript are indicated, and "ff." is used for following lines. I translated all transcripts from German to English. <back>
3) The social worlds of computer scientists, although involved in the social arena of the development of these HIV TOS, e.g., in taking care of day-to-day system administration, did not play a central role in this case study and will not be present in the following analysis. <back>
4) City names were changed for anonymization. <back>
5) All translations from German are mine. <back>
6) Here, the bioinformaticians acted in line with current ethical discourses in the development of medical ML tools, which are also concerned that the outcome produced by these tools should be explainable (BAUMGARTNER, 2021b). <back>
7) It is important to distinguish between the physician I interviewed who did not use HIV TOS and did not know a lot about them and the clinicians that have indeed been part of the development of the tools mentioned by the interviewed virologists and bioinformaticians. This second group will be interviewed in the future. Accordingly, in the social worlds/arenas map on Figure 1 a small overlap with the social world of bioinformaticians (for the few clinicians working on the development of HIV TOS) and a bigger one with virologists is depicted. <back>
8) I use the word "patients" as an in vivo code, when the social worlds are cited and when referring to people who started HIV treatment and were thus seen by different social worlds as a patient. To highlight a critical stance towards the term, the fixed role it assigned to people and the implications this role has had, I replace it with "people with HIV that seek treatment" or similar wording in other cases. <back>
9) People with HIV coming for treatment were not interviewed in this study. From my online and literature searches I assume, that some of them were organized in self-help groups. However, these groups were not mentioned by my interviewees and were not part of the development of the studied HIV TOS. <back>
10) Sanger is the traditional way of sequencing. NGS is the newer method, enabling a deeper look into the virus and a more complex picture of resistance probabilities. An ML tool developed by the same working group is available for NGS data (Bio1 and DS6). <back>
11) The boundaries of a category, as opposed to a classification, may be "fuzzy," and "membership [is] based on generalized knowledge and/or immediate context" (JACOB, 2004, p.528). <back>
12) In German Bio1 said "Versager," which I translated to "failure" or "loser." <back>
13) "Logic" is here used in the sense of a persisting rational or an appropriate style in the field as published by MOL (2008, p.1). <back>
14) Migration background is a category specifically used in the German context since race is considered a problematic category after the Nazi regime and its use is generally avoided. <back>
15) It is known that in the absence of professional(ized) interpreters (e.g, among new groups of immigrants to a place, where everybody knows everybody—and all their business), the code of ethical conduct which would otherwise ensure patient privacy can sometimes not yet have been established. This is justifiably experienced as gossip. However, this is a common feature of the early phases of any population’s migration to a new country, regardless of origin, and not something specific to migrants from Africa. <back>
16) A shared decision making between patients and physicians/medical experts is an ideal. This project analyzed power asymmetries between experts and patients within the arena of personalized HIV therapy. Coming from a power-critical stance, the question of to which extent patients should be involved in such decision-making processes and in more far-reaching questions around development of such tools might be raised. Bearing in mind the responsibilization of patients in certain arenas, such as PM, I wondered whether a new conceptualization of patients as informed actors could pave the way for more empowering and participatory processes of decision-making also within the development of such tools or the necessity of other tools instead. In this I echo the suggestion of Tina COOK, Helen ATKIN and Jane WILCOCKSON (2018) regarding participatory research for inclusive practice in the case of people with long term neurological conditions. <back>
Baumgartner, Renate (2021a). Precision medicine and digital phenotyping: Digital medicine's way from more data to better health?. Big Data & Society, 8(2), 1-12, https://doi.org/10.1177/20539517211066452 [Accessed: March 8, 2022].
Baumgartner, Renate (2021b). Künstliche Intelligenz in der Medizin: Diskriminierung oder Fairness?. In Gero Bauer, Maria Kechaja, Sebastian Engelmann & Lean Haug (Eds.), Diskriminierung und Antidiskriminierung: Beiträge aus Wissenschaft und Praxis (pp.147-162). Bielefeld: transcript.
Beerenwinkel, Niko; Schmidt, Barbara; Walter, Hauke; Kaiser, Rolf; Lengauer, Thomas; Hoffman, Daniel; Korn, Klaus & Selbig, Joachim (2002). Diversity and complexity of HIV-1 drug resistance: A bioinformatics approach to predicting phenotype from genotype. Proceedings of the National Academy of Sciences of the United States of America, 99(12), 8271-8276, https://doi.org/10.1073/pnas.112177799 [Accessed: March 7, 2022].
Beißwenger, Klaus-Dieter & Höpfner, Christine (1993). Aspects of AIDS and AIDS-HILFE in Germany. Berlin: Deutsche AIDS-Hilfe e.V.
Berger, Peter L. & Luckmann, Thomas (1969 [1966]). Die gesellschaftliche Konstruktion der Wirklichkeit. Eine Theorie der Wissenssoziologie. Frankfurt/M.: Fischer.
Blumer, Herbert (1969). Symbolic interactionism: Perspective and method. Berkeley, CA, USA: University of California Press.
Bosančić, Saša & Keller, Reiner (2019). Diskursive Konstruktionen. Eine Einleitung. In Saša Bosančić, & Reiner Keller (Eds.), Diskursive Konstruktionen: Kritik, Materialität und Subjektivierung in der wissenssoziologischen Diskursforschung (pp.1-8). Wiesbaden: Springer VS.
Clarke, Adele E. (1998). Disciplining reproduction: Modernity, American life sciences, and the problems of sex. Berkeley, CA: University of California Press.
Clarke, Adele E. & Montini, Theresa (1993). The many faces of RU486: Tales of situated knowledges and technological contestations. Science, Technology, & Human Values, 18(1), 42-78.
Clarke, Adele E. & Star, Susan Leigh (2008). The social worlds framework: A theory/method package. In Edward Hackett, Olga Amsterdamska, Michael Lynch & Judy Wcjam (Eds.), Handbook of science and technology studies (pp.113-137). Cambridge, MA: The MIT Press.
Clarke, Adele E.; Friese, Carrie & Washburn, Rachel (2015). Introducing situational analysis. In Adele E. Clarke, Carrie Friese & Rachel Washburn (Eds.), Situational analysis in practice. Mapping research with grounded theory (pp.11-76). Walnut Creek, CA: Left Coast Press.
Clarke, Adele E.; Friese, Carrie & Washburn, Rachel S. (2018). Situational analysis: Grounded theory after the interpretive turn (2nd ed.). London: Sage.
Clarke, Adele E.; Shim, Janet K.; Mamo, Laura; Fosket, Jennifer Ruth & Fishman, Jennifer R. (2003). Biomedicalization: Technoscientific transformations of health, illness, and U.S. biomedicine. American Sociological Review, 68(2), 161-194.
Cook, Tina; Atkin, Helen & Wilcockson, Jane (2018). Participatory research into inclusive practice: Improving services for people with long term neurological conditions. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 19(1), Art. 4, https://doi.org/10.17169/fqs-19.1.2667 [Accessed: April 11, 2023].
DAH – Deutsche AIDS-Hilfe e.V. (Ed.) (2005). Compliance: Umgang mit der HIV-Therapie. MED-INFO: Medizinische Informationen zu HIV und AIDS, 53, https://www.aidshilfe.de/shop/pdf/1060 [Accessed: February 15, 2023].
DAH – Deutsche AIDS-Hilfe e.V. (Ed.) (2010). Resistenzen. MED-INFO: Medizinische Informationen zu HIV und AIDS, 72.
DAIG – Deutsche AIDS-Gesellschaft e.V. (2020a). Deutsch-Österreichische Leitlinien zur antiretroviralen Therapie der HIV-1-Infektion. AWMF online, https://www.awmf.org/uploads/tx_szleitlinien/055-001l_Antiretrovirale_Therapie_der_HIV_Infektion__2021-06.pdf [Accessed: April 29, 2023].
DAIG – Deutsche AIDS-Gesellschaft e.V. (2020b). Deutsch-Österreichische Leitlinie zur HIV-Therapie in der Schwangerschaft und bei HIV-exponierten Neugeborenen. AWMF online, https://www.awmf.org/uploads/tx_szleitlinien/055-002l_S2k_HIV-Therapie-Schwangerschaft-und-HIV-exponierten_Neugeborenen_2020-10_01.pdf [Accessed: March 9, 2022].
Epstein, Steven (1996). Impure science: AIDS, activism, and the politics of knowledge. Berkeley, CA: University of California Press.
Erikainen, Sonja & Chan, Sarah (2019). Contested futures: Envisioning "personalized," "stratified," and "precision" medicine. New Genetics and Society, 38(3), 308-330.
European Medicines Agency (2018) [2007]. Atripla (Efavirenz/Emtricitabin/Tenofovirdisoproxil). Übersicht über Atripla und Begründung für die Zulassung in der EU, https://www.ema.europa.eu/en/documents/overview/atripla-epar-medicine-overview_de.pdf [Accessed: April 11, 2023].
Foucault, Michel (1974 [1971]). Die Ordnung des Diskurses. München: Hanser.
Fujimura, Joan H. (1987). Constructing "do-able" problems in cancer research: Articulating alignment. Social Studies of Science, 17(2), 257-293.
Gallo, Robert C. & Montagnier, Luc (2003). The discovery of HIV as the cause of AIDS. The New England Journal of Medicine, 349(24), 2283-2285, https://doi.org/10.1056/nejmp038194 [Accessed: April 11, 2023].
G-BA – Gemeinsamer Bundesausschuss (2004). HIV-Resistenztestung. Zusammenfassender Bericht des Arbeitsausschusses "Ärztliche Behandlung" des Bundesausschusses der Ärzte und Krankenkassen über die Beratung des Jahres 2003 zur Bewertung der HIV-Resistenztestung gemäß §135 Abs. 1 SGB V. Siegburg: Unterausschuss "Ärztliche Behandlung" des Gemeinsamen Bundesausschusses.
Jacob, Elin K. (2004). Classification and categorization: A difference that makes a difference. Library Trends, 52(3), 515-540.
Keller, Reiner; Hirseland, Andreas; Schneider, Werner & Viehöver Willy (Hrsg.) (2005). Die diskursive Konstruktion von Wirklichkeit. Konstanz: UVK.
Meuser, Michael & Nagel, Ulrike (2010). ExpertInneninterview. Zur Rekonstruktion spezialisierten Sonderwissens. In Ruth Becker & Beate Kortendiek (Eds.), Handbuch für Frauen- und Geschlechterforschung (pp.376-379). Wiesbaden: VS Verlag für Sozialwissenschaften.
Mol, Annemarie (2008). The logic of care. London: Routledge.
Offenberger, Ursula (2019). Anselm Strauss, Adele Clarke und die feministische Gretchenfrage. Zum Verhältnis von Grounded-Theory-Methodologie und Situationsanalyse. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 20(2), Art. 6, https://doi.org/10.17169/fqs-20.2.2997 [Accessed: March 8, 2022].
Poferl, Angelika (2004). Die Kosmopolitik des Alltags. Berlin: edition sigma.
Prainsack, Barbara (2017). Personalized medicine. Empowered patients in the 21st century?. New York, NY: New York University Press.
RKI – Robert Koch-Institut (2021). Aktuelle Daten und Informationen zu Infektionskrankheiten und Public Health. Epidemiologisches Bulletin, 47, https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/Ausgaben/47_21.pdf?__blob=publicationFile [Accessed: April 11, 2023].
Schmid, Sonja (2018). The discovery of HIV-1. Nature Milestones, 4, https://www.nature.com/articles/d42859-018-00003-x [Accessed: March 7, 2022].
Strauss, Anselm L. (1978). A social world perspective. Studies in Symbolic Interaction, 1, 119-128.
Strauss, Anselm L. (1984). Social worlds and their segmentation processes. Studies in Symbolic Interaction, 5, 123-139.
Strauss, Anselm L. (1993). Continual permutations of action. New York, NY: Aldine deGruyter.
Strauss, Anselm L. & Corbin, Juliet (1994). Grounded theory methodology: An overview. In Norman K. Denzin (Ed.), Handbook of qualitative research (pp.273-285). London: Sage.
Topol, Eric J. (2019). High-performance medicine: the convergence of human and artificial intelligence. Nature Medicine, 25, 44-56, https://www.nature.com/articles/s41591-018-0300-7 [Accessed: April 12, 2023].
|
Renate BAUMGARTNER works as post-doctoral researcher at the Center of Gender and Diversity Research at the University of Tübingen. She conducts research in (feminist) science and technology studies, especially on AI in healthcare and medicine. |
Contact: Dr. Renate Baumgartner Center of Gender and Diversity Research E-mail: renate.baumgartner@uni-tuebingen.de |
Baumgartner, Renate (2023). Personalized HIV treatment: Bringing marginalized patients to the forefront with situational analysis [48 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 24(2), Art. 23, https://dx.doi.org/10.17169/fqs-24.2.4083.

Creative Commons Attribution 4.0 International License