Volume 5, No. 2, Art. 2 – May 2004
Between Traditional and Scientific Medicine: A Research Strategy for the Study of the Pathways to Treatment Followed by a Group of Mexican Patients with Emotional Disorders
Shoshana Berenzon Gorn & Emily Ito Sugiyama
Abstract: The aim of this paper is to show how, on the basis of the social construction of reality and the informants' speech, it is possible to obtain original knowledge of the pathways to treatment of patients seeking to restore their mental health. The information presented is based on 13 people's verbal explanations of their pathways to treatment. According to Peter BERGER and Thomas LUCKMANN (1988), the language used by individuals in everyday life is the most effective means of transmitting meanings; it represents the objective accumulation of vast amounts of experience and meanings by this group. By extension, the language a group uses to talk about health constitutes its objectivized experience regarding this phenomenon at the same time as it serves to express it.
As in the theoretical aspect, the methodological aspect emphasizes the aim of constructing a spoken, participatory form of knowledge, which is why a qualitative methodology was used. The techniques used focused on non-participatory observation, field diaries and semi-structured interviews.
The interviewees' narrations and the observations carried out showed that the population has no problem combining various medical systems. The importance they place on each one depends, among other things, on their financial possibilities, logistic problems, their past experiences with the various systems, anecdotal information on the results obtained and the social networks available.
Key words: qualitative research on health, social construction of reality, pathways to treatment, emotional disorders, Mexico
Table of Contents
1. Introduction: Toward the Health's Comprehension
1.1 Normative and interpretative paradigms
1.1.1 Normative paradigm
1.1.2 Interpretive paradigm
1.2 Social constructionism and pathways to treatment
2. Method
2.1 Population
2.1.1 Approaching the informants
2.2 Undertaking the study
2.3 Analysis of information
3. The Interviewees
4. The Pathway to Treatment and the Complexity of Therapeutic Resources
5. Final Reflections
1. Introduction: Toward the Health's Comprehension
The aim of this paper is to show how, on the basis of the social construction of reality and the informants' speech, it is possible to obtain original knowledge of the pathways to treatment1) of patients seeking to restore their mental health. [1]
There is a wide range of medical practices in Mexico, resulting from the different historical, economic, cultural and social processes that the country has experienced that have gradually modified health care models. Rather than experiencing a dichotomy between traditional and scientific medicine, Mexico has a situation in which domestic, traditional, institutional and private medicine interact through their agents, such as doctors, psychiatrists, psychologists, homeopathic doctors, herbal doctors, midwives and folk healers. Moreover, the fact that government health services, private, traditional and domestic medicine intervene separately or together gives rise to a complex scenario that reveals a mixed health care system comprising several culturally integrated medical practices. [2]
The conceptualization of the health-sickness process in Mexico, including this mixed health care system, has existed since time immemorial. Thus, people have talked about natural and provoked ailments, spiritual and physical diseases and disorders of the body. The strategies or forms of intervention have also varied, and include magical-religious practices and surgical procedures, the use of medication or the properties of herbal medicine, therapies based on symbolic effectiveness and behavioral and psychiatric treatment, among others. [3]
1.1 Normative and interpretative paradigms
The models for approaching the study of health have also varied according to the dominant social schemes and scientific paradigms. This diversity in the methods of researching and understanding people and their world has yielded a rich, varied view of knowledge. [4]
Within the human and social sciences, there have been two main perspectives or ways of looking at the world, the positivist-objective and the anti-positivist-subjective approach. Within social psychology, this is usually referred to as the difference between the normative and the interpretative paradigm (PAEZ, VALENCIA, MORALES, SARABIA & URSUA, 1992). Each one of these perspectives is based on different theoretical and philosophical postulates, meaning that they propose different methodologies for approaching the study of health. [5]
Within the normative paradigm, the study of health is based on a clinical approach comprising three explanations: the anatomical-clinical one, which proposes an anatomical classification of illness, which only considers the moment when the wound appears and is expressed through signs, meaning that health is the absence of the latter. In the physio-pathological version, the concept of function arises as a reality regardless of the structure while the ethiopathological version is derived from the microbial theory of the origin of disease. During the 19th century, these versions were opposed to each other but by the early 20th century, they had been integrated into an eclectic version of disease (QUEVEDO, 1992). [6]
This clinical approach influenced the postulates of epidemiology, which states that disease is a reality of the structural and functional modification of organs, caused by different external agents, for example viruses, germs, drugs, pollution, etc., and now attempts are made to control these external agents. Environmental conditions intervene as elements that bring the agent into contact with the future patient. Both environmental conditions and microorganisms, signs, symptoms and changes in the body can be observed and measured. If the techniques used are appropriate, their behavior can be interpreted in statistical and quantitative analyses and eventually expressed in universal laws (QUEVEDO, 1992). [7]
Within this paradigm, there are various models that attempt to explain the use of health services. The most important of these include i) the epidemiological model; ii) the social learning model and iii) the economic model. A summary of their main characteristics is provided in Table 1.
|
Use of Health Services |
||
|
Epidemiological Model |
Social Learning Model |
Economic Model |
|
Based on the study of the population’s health needs. Damage to health (morbidity, mortality) constitutes the needs that motivate or induce the population to use the services. Use also depends on the population’s exposure to risk factors, which may be initiators, promoters and forecasts. The use of services is determined by the type of risk to which the population is exposed. Exposure to risk may imply a protective factor. The population "exposed" to a health service may be more "protected" than one which is not. |
Use understood as the activities undertaken by a person who thinks he is healthy in order to prevent illness. In order for this to happen, the following conditions must be fulfilled: a) The person must be psychologically prepared to carry out an action regarding a particular health condition. b) The individual must believe that prevention is feasible or appropriate in order to use it. c) There must be no psychological barriers to the proposed action. d) The presence of a "trigger" to produce the response. |
Based on the theory of human capital. Considers that use is linked to the demand for health, regarding it as a form of human capital in which one can invest. The cost of investing in health includes cash expenses and the opportunity costs of time (the optimal amount of investment depends on these two aspects.) Individuals inherit an initial store of health that depreciates over time. Health can be increased by investing in health services. Death occurs when the stock of health capital falls below a certain level. |
Table 1: Models about utilization services of health, normative paradigm (ARREDONDO & MELÉNDEZ, 1992) [8]
These ways of interpreting the process of health-disease have enabled certain immediate, individual problems to be dealt with. However, this paradigm begins to break down because of its inability to explain the relation between illness and society, seen within an integral context in which man as a social being is the main actor and where obviously all his actions concerning the environment, forms of production, the way of relating to other men and to oneself are determining historical processes within which the concept of health and disease is framed (QUEVEDO, 1992). [9]
In addition to the above, within this paradigm, a bias was introduced into the approach to social reality and health by focusing exclusively on illnesses recognized within the dominant medical paradigm. Thus, certain problems that are difficult to deal with ideologically, operatively or culturally, such as fear, malnutrition or alcoholism, are relegated to oblivion (LUZ, 1999). [10]
These criticisms are based on various economic, demographic, historical and sociological studies that confirm the fact that "diseases" have changed throughout history, meaning that certain common forms of illness have been modified or even disappeared while other new ones have appeared, due to transformations of social and economic organization and the demographic behavior of communities. Likewise, anthropology has shown that individuals' response to a particular process of change is not always the same and that there are cultural elements that influence the perception of symptoms and behavior towards them. In other words, the socio-cultural context interacts with the genetic, the biological and the psychic in the process of organizing the forms of presentation, representation and modification of an individual's life processes (BREILH, 1994). [11]
A number of criticisms have also been made of the methods used within this paradigm. In this respect, Mario BRONFMAN, Roberto CASTRO, María Elena ZÚÑIGA, Carlos MIRANDA and Jorge OVIEDO (1997) posit that because of the characteristics of the research methods and techniques used, it is difficult to explore aspects that enable one to understand why certain health services are used, what determines the use of services, or what elements or factors underlie the decisions made by individuals, among many other issues. [12]
In response to these criticisms, the interpretive paradigm understands the process of health-illness as part of everyday life, as a result of which the latter is mediated by social, cultural and historical relations, which implies a "community" view in which individuals express themselves separately and collectively. Thus, health is no longer understood as a state; it is a process of permanent construction that recognizes cultural and social aspects as symbolic, material expressions that comprise all man's relationships and therefore his life itself. [13]
Within this same order of ideas, Francois LAPLANTINE (1986) notes that health and disease are privileged objects within culture, firstly because they are notions that enable one to grasp the different forms of coordination between the individual and the social, between personal experience and social structure. Secondly, they are located within the field of the intersection of values (they imply evaluations of this knowledge and practices) and the field of action (they determine behavior). Thirdly, they are events that modify our individual lives, our insertion in society and thereby, collective equilibrium. They also invariably entail the need for a discourse involving the complex, continuous interpretation of society as a whole (VIVEROS, 1993). [14]
For his part, Roberto CASTRO (2000) notes that interpretive approaches highlight actors' capacity to lend meaning to different social situations and to act rather than merely "react" as a result. Interpretive trends analyze the specific ways in which individuals feel, perceive and define the different aspects of social life, in such a way that they are transformed into significant experiences for them, in other words, they begin with the direct exploration of people's testimonies. [15]
One of the positions include in the interpretive paradigm is social constructionism. This theoretical model does not accept the existence of a single model of health and illness, but rather a wide range of particular systems, which in turn are determined by cultural diversity (GUTIÉRREZ & VILLA DE PINEDA, 1995). [16]
On the basis of the above, we begin with the idea that the phenomenon of health is complex and can therefore be studied from various approaches or perspectives. However, it is also quite clear to us that any knowledge of this phenomenon is relative, in other words, it is not isolated from other knowledge, nor is it sufficient in itself nor can it exist on its own. In other words, knowledge is not absolute, which leads one to posit that there are no universals regarding illness and health, in the sense of generalizing a truth that ignores the specific or particular characteristics of different human groups (MADURO, 1992). This is how we propose social constructionism as a means of interpreting the pathways to treatment followed by patients with emotional disorders. [17]
1.2 Social constructionism and pathways to treatment
Social constructionism is based on the idea that reality, including science, is a socio-cultural construction. From this perspective, the construction of reality is achieved through symbolic interaction and the everyday practice of persons, who find their basis in a local-cultural moral order that is created and reproduced in the micro-social exchange (MEDINA, 1994). [18]
Kenneth GERGEN (1985) has defined social constructionism as a type of research linked to intellectual trends such as symbolic interactionism, symbolic anthropology, ethnomethodology, literary deconstructionism, phenomenology, existentialism and certain theories of social psychology. All of these share the conception that the subject plays an active role, guided by his culture, in the structuring of reality This research perspective is therefore considered "endogenic" or generated by the subject himself, in contrast with the use of "exogenic" perspectives that are outside the subject's construction of his reality (TIEFER, 1987). [19]
This theoretical position examines the influence of social groups on the origin and evolution of illnesses and the diagnosis and treatment of the latter. Illnesses are explained by the structure of meanings, which, within a set cultural context and at a given moment, subjects assign to health and illness. Society's points of view not only influence the definition or meaning of the disorder but also intervene in the treatment and prognosis of the latter. For example, in certain Mexican cultures, an adult who is caught doing something improper and is ridiculed suffers from "shame," a disease expressed through the swelling of the legs, which can only be treated by a traditional community therapist (PAEZ et al. 1992; ARREDONDO & MELÉNDEZ, 1992; COMELLES & MARTÍNEZ, 1993). [20]
In the analysis of health services, the constructionism perspective emphasizes the importance of socio-cultural and environmental aspects in the construction of meanings around health services and in the choice of one or more therapeutics. In this respect, the use of a specific medical2) system is largely determined by the individual's personal history, the onset of the illness3), the context in which the disorder appears, the social legitimacy of the latter, and the legitimacy of the therapeutics. Both forms of legitimacy are provided by the subject's approval and valuation within the social context (ARREDONDO & MELÉNDEZ 1992; MARTÍNEZ, 1995; VARGAS & CASILLAS, 2000). [21]
María Eugenia MÓDENA (1999) points out that medicines and medical systems refer to the whole of technical knowledge, the practices, representations and set of institutions, healers, philosophies and worldviews that underlie these systems, impressing on them the fundamental characteristics of the conception of man, his health and his diseases, among other things. [22]
In addition to the above, in any medical system, the beliefs and behaviors comprising curative practices are influenced by specialized scenarios (surgeries, rooms, etc.) personal relations (healer-patient, patient and his family group, patient and his network of social relations), political restrictions (regulations, permits), financial restrictions (cost of treatment, cost of service), treatment and available interventions (knowledge, resources, access to technology) and the types of health problems, among many other factors (MÓDENA, 1999). [23]
On the basis of this plurality of medical systems, María Eugenia MÓDENA (1999) proposes a different way of conceptualizing the alternative. According to MÓDENA the alternative refers to the simultaneous combination of resources. This attention strategy usually refers to a greater complexity that is socially constructed and comprises the causality, symptoms, signs and meanings of illnesses, becoming part of the illness. The simultaneous combination of various health systems is intended to deal with various aspects of a single disease or various illnesses or processes that require attention but have been triggered by a single factor. An accident, for example, can simultaneously cause a fracture and "a fear attack." In this example, two different types of attention are required, since each one satisfies a different aspect within the cultural complexity that this event represents. This is supported by Gloria GARAY and Carlos PINZÓN (1997) who posit that, in order to analyze the use of "various medicines" it is necessary to abandon the aim of finding a single logic. They note that it is even possible to find contrasting or juxtaposed forms of logic within a single therapeutic trajectory. [24]
Social constructionism theorists posit that the construction of illness and health, the choice of a particular service and the pathway to treatment are achieved through the symbolic interaction and everyday practice of people who find their basis in a moral, social, local, institutional and cultural order that is created and reproduced in the microsocial exchange (MEDINA, 1994). In other words, individuals, in their everyday lives, participate with others in a shared knowledge and an interpretation of reality that is common to all and enables them to communicate. This microsocial exchange presupposes processes of interaction and communication, through which the experiences of other people, and the events and objects of any health system are grasped through typifying schemes that become progressively anonymous insofar as they move away from the here and now. In other words, knowledge is constructed and reconstructed not only with and through one's fellow human beings, with whom direct interaction is established, but also with one's contemporaries and not only them, but with one's predecessors and successors (BERGER & LUCKMANN, 1988). [25]
Thus, medical or curative knowledge circulates as anonymous evidence, regardless of the men and situations that created it. It is knowledge or rather a given reality and therefore the possibility of existence and reproduction in everyday life. It exists insofar as human expressiveness manages to be concentrated, crystallized or objectivized in signs, symbols or meanings grouped together in systems which are objectively accessible. Language constitutes the system of signs between human beings. It permits the social accumulation or collection of knowledge "which is transmitted from generation to generation and is within the individual's reach in everyday life" (BERGER & LUCKMANN, 1998, p.62). [26]
According to the postulates we have pointed out, an interpretive analysis was proposed based on the verbal explanations of 13 people and on the observations (explained in the field notes) made by the researchers, since it is assumed that the language used in everyday life is the most effective means of transmitting meaning. Language is the means through which interpretive activity can be observed (BERGER & LUCKMANN, 1998). By extension, the language that a group uses to discuss health and health services constitutes the objectivized experience of this group regarding these phenomena, at the same time as it serves to express it (CASTRO, 2000). [27]
In keeping with the constructionist theory, the first step consisted of posing questions about the human experiences concerning health, illness and treatment resources that the study sought to explore. Subsequently, the techniques and sources for collecting the information were selected, which focused on non-participatory observation, field diaries, and semi-structured interviews (ALONSO, 1995). The interviewers experiences were added to this, in order to achieve a broader view of this process of constructing meaning (GOETZ & LE COMPTE, 1991). [28]
The latter means that knowledge was built throughout the research process. Consensus about the conclusions was attained through dialogue, interaction and direct experience, which implied continuous observation and reflection processes as well as the construction of shared meanings and systematization. The different meanings constructed about health, illness and the use of diverse health systems were accomplished on the basis of joint efforts from the research team and social actors. [29]
As mentioned earlier, 13 people who said that either they or a close relative (usually one of their children) suffered from a particular emotional disorder were observed and interviewed. Cases were selected using the theoretical sampling strategy proposed by Barney GLASER and Anselm STRAUSS (1967) where the information provided to interpret the subject or topic of interest is more important than the number of people interviewed. The aim of this type of sampling is to obtain information that will complement what is being researched. The process, known as saturation, ends when interviews with additional people fail to yield any new or relevant information regarding the phenomenon. [30]
2.1.1 Approaching the informants
Interviewees were contacted through the "snowball" technique, a particular form of chain analysis that seeks to construct a sample of individuals with common characteristics within a wider universe (TROTTER & MEDINA-MORA, 2000). In this case, the first folk healer contacted served as an agent for locating cases, by introducing the researchers to other folk healers who in turn, put us into contact with those that used their services. [31]
Once contact had been established, the researchers gave a presentation, through which they attempted to establish a relationship of trust and honesty with the informant. In order to achieve this, it was necessary for the researchers to reveal their real interest in him. They told the interviewee about the reasons for the interview, the confidential nature of the data, and asked for his permission to record the interviews and to publish the information obtained.4) At the end of the interview, the interviewee was thanked for his cooperation, reminded of how useful the information would be and asked for his opinion on the interview. [32]
The interviews, which required face-to-face interaction, lasted approximately two hours. Some interviews were completed in a single session whereas in other cases, one or two additional sessions were required. The time used to transcribe each interview was approximately six hours. [33]
In order to carry out the fieldwork, two stages of fully interrelated stages of research were constructed. The first phase involved a series of observations with an ethnographic approach. During the second phase, conversations were held with selected informants, using the social interview technique (GALINDO, 1987; SIERRA, 1998).
First Phase: Two different types of observation were carried out; exploratory and descriptive (GALINDO, 1987). The exploratory observations were undertaken on each of the field trips. The notes obtained during these observations provided an overview of the areas where the interviewees were located. The interviewers noted both the characteristics of the place and the interviewees' contact with certain people. In each of the encounters with the interviewees, descriptive observations were made, in far more detail. It is important to mention that although each researcher had his or her own personal way of taking field notes, certain criteria were suggested to ensure that all the notes included basic information.
Second Phase. The social research interview was the other technique used to obtain the narrations (ALONSO, 1995). In order to compile the information, an interview guide was drawn up with the following key themes: 1) Clinical history of disorder; 2) pathway to treatment (persons or services sought by patient; period and order in which they attended, reasons for using or not using the various persons or services, differences and similarities between the persons and services visited, 3) account of treatment by folk healer (first contact with folk healer; treatment received, perceptions and impressions of treatment received; 4) social and cultural perception of mental health 5) socio-demographic data. [34]
The interviewees' accounts constituted the basis on which the analysis of this study was carried out. In other words, the meanings that the interviewees attached to illness, the ways in which they were experienced and the treatment provided. We began with the idea that the informants are the ones who "know most." However, in our role as researchers, we would like to mention the fact that the challenge in this research was "to say something more" by linking and interpreting the narrations produced by the interviewees in light of our theoretical frame. [35]
All the interviews were transcribed in order to subsequently be able to compare the audio-taped records with the written records and correct any possible errors. After the interviews had been read through several times, a series of categories was drawn up in order to classify the information from the subjects dealt with in the conversations. This grouping was based on the "categorization of meaning" technique proposed by Steinar KVALE (1996). [36]
Through this technique, each interview is encoded in a series of mutually exclusive categories, enabling one to break down extensive, complex narrations into smaller classifications. This procedure facilitates the understanding of a particular phenomenon and its occurrence throughout the interview, in addition to facilitating the description of the most important characteristics of the content. [37]
The analysis categories were identified on the basis of the objectives proposed in the interview guide and each of them was perfectly defined in order to facilitate the encoding process. In order to identify possible differences of criterion during this process and to reach a consensus on the most suitable categories, two people separately codified the same material and subsequently compared their categorizations (KVALE, 1996). [38]
Once this categorization had been carried out, the next step consisted of categorizing each subject in more detail. Unlike the first codification process, which was carried out deductively (the subjects were determined on the basis of the work objectives), the second stage of codification of each subject was carried out inductively, since the successive readings of each interview enable the information contained in each one to be recognized. This process of codification enabled the categories that were best suited to the information that had been compiled to be constructed, which in turn facilitated the interpretation and analysis of the testimonies on the basis of the theoretical frame used. [39]
Finally, the categories produced were studied as a whole in conjunction with the whole text and an analysis was carried out of the way in which each interview was determined by the culture of the informants, the sensitivity of the topic and their knowledge of the latter and the spatial and/or temporal setting in which the interview was carried out, in other words, the interviewees' speech in their context was studied (ALONSO, 1995). [40]
The information obtained at the end of the research is the result of a series of transformations. The observations compiled were transformed into texts and an analysis was carried out of this written material. In the case of the interviews, the transformations began at the time of the recording and ended with the process of analysis. The interviews were initially recorded, which enabled what had been said to be preserved, in other words, rescued from its perishable form and preserved in a way that could be consulted (GEERTZ, 1992). However, some of the features inherent in speech such as gestures or facial expressions are lost in audio-tapes. The second transformation occurred when the content of the recording was converted into written text. During this conversion, inherent aspects of speech, such as intonation, volume, tone and timbre are lost. An additional transformation took place during the process of categorization and the last transformation took place at the moment of analysis and interpretation, when the categories were converted into meanings (CASTRO, 1996). [41]
This theoretical and methodological strategy was used to systematize the information compiled during the interviews and observations. This method made it easier to understand the way patients understand and experience their pathways to treatment and to estimate the importance of the latter for the social actors involved. [42]
Thirteen people (9 women and 4 men) were interviewed. In order to ensure the confidentiality of the information provided, fictitious names were used. Most of the informants were aged between 30 and 50. All of them live in the Federal District, although not all of them are originally from Mexico City. Seven of the thirteen interviewees are practicing Catholics, three are atheists and the remaining three said that they believe in God. The interviewees engage in extremely diverse professions and activities and include businessmen, housewives, professionals and civil servants. As for their level of educational attainment, three completed primary school, and one completed secondary school, five completed high school and four hold university degrees. [43]
Each of the interviewees was asked about the history of his or her disorder, in other words, the characteristics and development of the latter, as well as the point when they decided to request some type of assistance and the reasons that had led them to choose a particular option. They were also asked to mention the name of the disorder, on the basis of the meaning they gave it rather than on the basis of the diagnosis or name given by any of the doctors, healers, or health care providers consulted. [44]
Four informants cited family, work and/or financial problems as the factors that had led them to seek some type of help. Three of the interviewees said that they suffered from physical disorders derived from a particular emotional disorder (such as nervous colitis, throat problems, etc.) while two of them said that the main reason was that they felt depressed. The remaining four requested some type of help in order to solve emotional problems as a result of illnesses suffered by close relatives. [45]
4. The Pathway to Treatment and the Complexity of Therapeutic Resources
As mentioned in the introduction, for the purposes of this study, pathway to treatment is understood as the set of activities, persons consulted and health services requested by a person or his immediate social environment (family, partner, friends, etc.) in search of a solution, cure or relief for an ailment. The search is regarded as having been completed when a person's health has been restored or when the impossibility of a cure has been confirmed and accepted. [46]
It is worth mentioning that each of the interviewees has her/his own history, a subjective experience of her/his suffering and a strategy for coping with suffering. What they all share is the recognition of various medical systems as possible alternative solutions to health problems. [47]
As one can see from Table 2, most of the patients interviewed combine and try out various medical options by constructing numerous alternatives and strategies in the quest for health. Only five of the interviewees reported using home remedies. Eight of the patients initially sought help from a general practitioner or family doctor; two were seen by mental health professionals while the remaining three resorted to a traditional doctor. Most of the interviewees subsequently sought other means of support, which are complementary rather than exclusive. In other words, they resort at the same time to alternative services, mental health specialists and other specialized doctors in order to complete the sequence of the pathway to treatment with a traditional doctor, a scientific doctor or both.
|
Interviewee |
Disorder |
Pathways to treatment |
|
Marcela |
Family problems |
|
|
Mister K |
Work and family problems |
|
|
Marco |
Family problems Drug use |
|
|
Sergio |
Financial problems |
|
|
Susana |
Depression, sadness
|
|
|
Beatriz |
Depression, sadness |
|
|
Claudia |
Stress |
|
|
Ximena |
Nervous Colitis |
|
|
Gabriela |
Nervous Colitis |
|
|
Mercedes |
Emotional disorders |
|
|
Sara |
Emotional disorders. |
|
|
Natalia |
Emotional disorders
|
|
|
Eduardo |
Emotional disorders |
|
Table 2: Summary of the pathways to treatment followed by patients5) [48]
The sequence described in the Figure 1 is the characteristics of most of the patients' pathway to treatment, with no significant differences appearing between the various types of disorder.
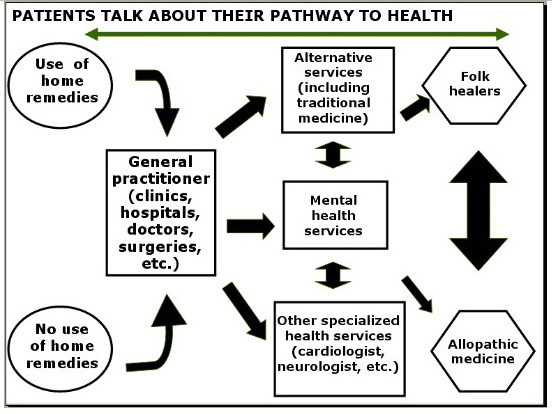
Figure 1: Pathways to health [49]
According to the interviewees' testimonies, they initially opt for a particular type of service, but once they see that their health expectations are not fulfilled, they look for another method that will prove more effective. The search is regarded as having been concluded when they feel that their health has been restored or at least when they are given a satisfactory response to their suffering, even when the impossibility of a cure has been confirmed. The informants agree that there is no contradiction between the choice of a particular form of health care, and that they all coexist "naturally" as possibilities or real supplies, in other words, no medical practice is discarded or disqualified. [50]
The combination of services chosen and the importance given to each of them depends, among other things, on the resources available to a person for health care (financial, geographic, social security, etc.), the possibility of reinterpreting and using the information on the various systems of health care on the basis of previous experiences, anecdotal information on the results obtained and the way in which the illness is conceptualized. [51]
This combination of various medical systems has at least two functions. The first has to do with the possibility of creating a set of possible options and thereby maximizing curative resource. The second, according to María Eugenia MÓDENA (1999) is that the use of various health resources has the function of satisfying and dealing with different aspects of the same illness in which a single medical system is unable to satisfy the cultural complexity of the event. [52]
The following account exemplifies this second function, in that Mercedes began to resort to various alternatives as a result of her daughter's illness. The interviewee simultaneously sought a cure for her daughter and an answer to what was happening that would soothe her and relieve her from guilt. In this respect, a satisfactory response will not only have to do with the effectiveness of the treatments or the degree of improvement of her daughter's problem but also with the coincidence between this response and the interviewee's experiences and her beliefs about the illness.
"When my youngest daughter was 6 months old, she was diagnosed with cerebral palsy at the National Institute of Children's Disease (DIF). At that point I panicked and went into an emotional and existential crisis. It took me several years to work out my position and understand my daughter's problem, and during that time, I went out with one person after another. I went to spiritual cleansing sessions, saw witches and went to séances. I've tried plants and plant therapy, microdoses and Bach flowers. I took refuge in religion. I took my daughter to several institutions and to a little school for children like her. I have also consulted psychologists and physiotherapists. I've tried homeopathy and Reiki. It is as though life was pushing me in one direction after another. I've just come back to the DIF, meaning that I have come the full circle. I've come back to the DIF where they have had a physiotherapist ever since my daughter was 14 and that has helped a lot, my daughter has made a great deal of progress with her.
During my various searches, I have discovered things that have proved extremely useful, that have calmed me down and that have made me grow and mature and enabled me to see my daughter as she is, not as a sick person.
I'm interested in and enthusiastic about going on searching, but it has become a sort of passion that has nothing to do with my daughter, but rather about knowing more and finding alternatives and discovering what is happening and all that. For example, at the moment I'm into holistic medicine. The doctor gives me capsules but I don't know what's in them. But what moves me is faith because I think that, as long as God gives me health and strength, I should go on searching to find the right path. Because that's what life Is, it's a learning process, a search, that's what I think, you have to go on searching." (Mercedes) [53]
The theoretico-methodological strategy chosen was a useful tool for recovering the field of the word and language, awareness, beliefs and will, which allowed us to explore the links between the subjective experience of health, illness, the various health systems and the environment within which this experience is produced. It also showed that the understanding of meanings is deeper when it is dealt with from the perspective of its principal actors, in this case, the service users. [54]
As mentioned in the theoretical framework, dealing with the subjective experience of the health-illness process from the normative paradigm has several limitations, one of which being that it focuses on observable phenomena, such as people's behavior when they use services. This study utilized the perspective proposed by social constructionism, in which greater importance is given to language or to what is said as a means of transmitting knowledge with a social origin, which provided another means of analysis of the way in which the meanings of experiences are constructed towards therapeutic resources. [55]
Likewise, the constructionist perspective adopted in this research allowed for setting up a link between "macro" and "micro." This in turn made it possible to articulate individual and social aspects, individual experiences and social structure (LAPLANTINE, 1986; PAEZ, 1992; ARREDONDO & MELÉNDEZ, 1992). According to CASTRO (2000), folk healers and patients' narratives about health, illness and service utilization reflect the interviewee's subjective experience related to such issues as well as some information regarding the common social relationships of their group. The reasons for seeking help in different medical systems are clear examples. People seek help in order to re-establish the equilibrium they lost due to the negative emotional and psychological effects of urban lifestyle; when the problems posed threaten their cultural identity and/or gender roles, and when they try to find solutions for illnesses. This type of illnesses is the result of the constant economical, social and moral crisis that the Mexican population has and is still experiencing. In other words, suffering such health problems is not only the consequence of a biological process or the result of an unfortunate personal history, but the result of many experiences lived here and now, within a social system where the population is integrated. [56]
In conjunction with the above, this approach has enabled us to construct a form of knowledge that incorporated both the perspective (knowledge and feeling) of those that know (the patients) and of those who were trying to find out (the researchers). In other words, we managed to establish a dialog between different types of knowledge, understood as a symbolic-cultural dialog that is nothing more than the possibility of mutual understanding. This relation is only possible on the basis of the rationality of the argumentative discourse that links and creates by agreeing with certain aspects, discerning others, negotiating, convincing and allowing oneself to be convinced (ALBA & PINZÓN, 1997). [57]
It is worth noting that various medical systems are combined, complemented and juxtaposed in the pathways to treatment followed by the patients interviewed. Although patients may criticize and make value judgments about the services, but it does not prevent them from using the services at the same time. This coincides with what we have found in other studies (GUTIÉRREZ & VILLA DE PINEDA, 1995; ZOLLA, DEL BOSQUE, MELLADO, & TASCÓN 1992, CABIESES, 1996; BRONFMAN et al., 1997; MÓDENA 1999) in the sense that, regardless of their type of suffering and their financial position or educational attainment, people resort to all the possibilities available to them to find a cure or at least a satisfactory response to their problem. Resorting to various medical systems is a common practice among the population and fulfills specific functions. [58]
The information included here contributes elements to the undeniable social fact that there is a syncretism of medical practices. The population resorts to all the possibilities it has available in the search for attaining health. Thus, official or scientific medicine coexists with traditional medicine, acupuncture, and other ways of dealing with illnesses and ailments such as homeopathic medicine or spiritualism. Likewise, it makes one realize that resorting to medical systems other than the official one has nothing to do with the population's ignorance or with the lack of services or safety, or with a person's socio-economic status or level of educational attainment. Resorting to other medical traditions has more to do with the way suffering is interpreted. [59]
Lastly, the results of this study evince the need for a pluralistic health system that will offer the population more therapeutic options as a response to its needs and demands. As Julio PAYÁN posits (1998), one should not think that, under this model, official science should absorb other medical knowledge or "approve" it, like an indulgent parent, since every type of knowledge has its own cultural, social and political recognition. The aim is to establish a climate of respect towards different types of knowledge that will lead to greater possibilities for everyone. [60]
The authors of this paper would like to thank the interviewees who shared their knowledge and experience with us and made this study possible.
1) In this study, pathway to treatment is understood as the set of activities, people consulted and services requested by a person or his immediate environment (family, partner, friends, etc.) in search of a solution, cure or relief from a problem. The search is regarded as having been concluded when the patient feels that his or her health has been restored or when the impossibility of a cure is confirmed and accepted. <back>
2) A medical system is a complex of ideas about the causes and cures of illness, none of which is entirely rational or irrational. The practices and most of the curative procedures are understandable and logical in the light of the nature of health and causes of illness. They are also integrated parts of the culture, which are affected by other categories such as economy, religion and education. Every medical system includes beliefs that promote health, stock and the scientific knowledge and the group members' ability to subscribe to them (GUTIÉRREZ & VILLA DE PINEDA, 1995). <back>
3) It is the set of meanings that a person gives to an event that befalls him and the consequences of the latter for him and his social setting. Suffering is the subjective view of illness, it is the set of psychic and social repercussions of an illness. These meanings are not inherent, but constructed around each individual with different social groups. In other words, it is a popular, everyday form of knowledge, meaning that what a particular group classifies as an illness makes a person from this group feel or regard himself as sick. It also affects the way in which actions carried out by doctors, healers and self-help groups are valued and interpreted. Likewise, the religious and magical practices adopted by this social group determine the way illness and healing are interpreted (MARTÍNEZ, 1995; VARGAS & CASILLAS, 2000). <back>
4) Qualitative research observes three ethical principles: informed consent, guarantee of anonymity, and protection from the abusive exercise of power in the relation between researcher and participant (PARIS, 1999). <back>
5) Fictitious names are used to preserve anonymity. <back>
Alba, David & Pinzón, Maritza (1997). Reflexiones metodológicas para abordar la dimensión cultural en el desarrollo local [Methodological Reflections to Discuss the Cultural Dimension in Local Development]. Paper delivered at the VIII Congress of Anthropology in Colombia, Colombia University, Santa Fe, Bogotá, December 5-7.
Alonso, Luis (1995). Sujeto y discurso: El lugar de la entrevista abierta en las prácticas de la sociología cualitativa [Subject and discourse: The Place of the Open Interview in the Practice of Qualitative Sociology]. In Juan Delgado & Juan Gutiérrez (Eds.), Métodos y técnicas de investigación en ciencias sociales (pp.225-240). Madrid: Síntesis.
Arredondo, Armando & Meléndez, Víctor (1992). Modelos explicativos sobre la utilización de servicios de salud: revisión y análisis [Explicative Models for the Use of Health Services: Review and analysis]. Salud Pública de México, 34, 36-49.
Berger, Peter & Luckmann, Thomas (1988). La construcción social de la realidad [The Social Construction of Reality]. Buenos Aires: Amorrourtu.
Breilh, Jaime (1994). Nuevos Conceptos y Técnicas de Investigación en salud. [New Concepts and Research Techniques in Health]. Quito: CEAS.
Bronfman, Mario; Castro, Roberto; Zúñiga, Elena Zúñiga; Miranda, Carlos & Oviedo, Jorge (1997). "Hacemos lo que podemos": los prestadores de servicios frente al problema de la utilización ["We do what we can": Health Service Providers Faced with the Service Use Problem]. Salud Pública Mex, 39, 546-553.
Cabieses, Fernando (1996). La articulación de las medicinas tradicionales con la medicina oficial [Linking Traditional Medicine to Official Medicine]. Anales de la Facultad de Medicina de la Universidad de San Marcos, 57, 12-18.
Castro, Roberto (1996). En busca del significado: supuestos, alcances y limitaciones del análisis cualitativo [In Search of Meaning: Assumptions, Scope and Limitations of Qualitative Analysis]. In Ivonne Szasz & Susana Lerner (Eds.), Para comprender la subjetividad; investigación cualitativa en salud reproductiva y sexualidad (pp.57-87). México: El Colegio de México, Centro de estudios demográficos y desarrollo urbano.
Castro, Roberto (2000). La vida en la adversidad el significado de la salud y la reproducción de la pobreza [Life in Adversity. The Meaning of Health and the Reproduction of Poverty]. México: Centro Regional de Investigaciones Multidisciplinarias, Universidad Nacional Autónoma de México.
Comelles, Josep & Martínez, Ángel (1993). Enfermedad, Cultura y Sociedad. Un ensayo sobre las relaciones entre la Antropología Social y la Medicina [Illness, Culture and Society. An Essay on the Relations between Social Anthropology and Medicine]. Madrid: Edudema.
Galindo, Jesús (1987). Encuentro de subjetividades, objetividad descubierta. La entrevista como centro del trabajo etnográfico [Encounter between Subjectivities, Objectivity revealed. The Interview as the Center of the Ethnographic Study]. Revista de la Universidad de Colima, 1, 151-183.
Garay, Gloria & Pinzón, Carlos (1997). Salud y subjetividad urbana [Health and Urban subjectivity]. Paper delivered at the VIII Congress of Anthropology in Colombia. University Colombia. Santa Fe, Bogota.
Geertz, Clifford (1992). Géneros confusos. La refiguración del pensamiento social [Confused genders. The Reconfiguration of Social Thought]. In Carlos Reynoso (Ed.), El surgimiento de la antropología postmoderma (pp.187-211). Mexico: Gedisa.
Gergen, Kenneth (1985). The Social Constructionist Movement in Modern Psychology. American Psychologist, 40, 266-275.
Glaser, Barney & Strauss, Anselm (1967). The Discovery of Grounded Theory. Chicago: Aldine.
Goetz, Judith & Le Compte, Margaret (1991). Etnografía e investigación cualitativa [Ethnography and Qualitative Research]. Madrid: Morata.
Gutiérrez, Virginia & Villa de Pineda, Patricia (1995). Medicina Tradicional de Colombia [Traditional Medicine in Colombia] (Vol. 2). Bogotá: Presencia Ltda. Public.
Kvale, Steinar (Ed.) (1996). Methods of Analysis. London: Sage Publications.
Laplantine, Francois (1986). La etnopsiquiatría [Ethnopsychiatry]. España: Gedisa.
Luz, María (1999). Cultura contemporánea y medicinas alternativas: nuevos paradigmas en salud al finalizar el siglo XX [Contemporary Culture and Alternative Medicines: New Paradigms in Health in the Late 20th Century]. In Mario Bronfman & Roberto Castro (Eds.), Salud, cambio social y política.Perspectivas desde América Latina (pp.363-382). Mexico: EDAMEX.
Maduro, Otto (1992). Mapas para la fiesta. Reflexiones Latinoamericanas sobre la crisis y el conocimiento [Maps for the Party. Latin American Reflections on the Crisis and Knowledge]. Río de Janeiro: Centro Nueva Tierra.
Martínez, Fernando (1995). El hombre y su padecer, centro de una nueva medicina [Man and His Suffering, the Center of New Medicine]. Médico Moderno, XXXIV, 11-86.
Medina, Raúl (1994). El estudio de la familia: nuevas direcciones de investigación psicosocial [The Study of the Family: New Directions in Psychosocial Research]. Revista de la Universidad de Guadalajara, 3, 64-70.
Módena, María Eugenia (1999). Cultura, enfermedad-padecimiento y atención alternativa. La construcción social de la desalcoholización [Culture, Illness, Suffering and Alternative Care. The Social Construction of De-alcoholization]. In Mario Bronfman & Roberto Castro (Eds.), Salud, Cambio Social y Política. Perspectivas desde América Latina (pp.382-401). México: EDAMEX, INSP.
Paez, Dario; Valencia, José; Morales, José; Sarabia, Bernabé & Ursua, Nicanor (1992). Teoría y Método en psicología social [Theory and Method in Social Psychology]. Madrid: Anthropos.
Paris, Mary (1999). Investigación Cualitativa en salud: superando los horrores metodológicos [Qualitative Research in Health: Overcoming Methodological Horrors]. In Mario Bronfman & Roberto Castro (Eds.), Salud, Cambio Social y Política. Perspectivas desde América Latina (pp.35-47). México: EDAMEX, INSP.
Payán, Julio (1998). Posibilidades de un diálogo entre saberes [Possibilities of a Dialogue between Types of Knowledge]. Revista de Medicina Holística, 42, 1-12.
Quevedo, Emilio (1992). El proceso de salud-enfermedad: hacia una clínica y una epidemiología no positivista [The Health and Illness Process: Toward Non-Positivist Clinical Medicine and Epidemiology]. Bogotá: Zeus Asesores Ltda.
Sierra, Francisco (1998). Función y sentido de la entrevista cualitativa [Function and Meaning of the Qualitative Interview]. In Jesús Galindo (Ed.), Técnicas de investigación en sociedad, cultura y comunicación (pp 277-341). Mexico: Addison Wesley Longman.
Tiefer, Leonore (1987). Social Constructionism and the Study of Human Sexuality. Newbury Park, CA: Sage.
Trotter, Robert & Medina-Mora, Ma Elena (2000). Qualitative methods. In World Health Organization (Ed.). Guide to Drug Abuse Epidemiology (pp.93-124). Ginebra: World Health Organization.
Vargas, Luis & Casillas, Leticia (2000). El efecto del padecer sobre el individuo-persona y el riesgo de transformar al paciente en sujeto u objeto [The Effect of Suffering on the Individual-person and the Risk of Turning the Patient into a Subject or Object].Ciudad de México: Universidad Nacional Autónoma de México, Instituto de Investigaciones Antropológicas y Facultad de Medicina.
Viveros, María (1993). La noción de representación social y su utilización en los estudios sobre salud-enfermedad [The notion of Social Representation and its Use in Studies on Health-Illness]. Revista Colombiana de Antropología, 30, 239-260.
Zolla, Carlos; Del Bosque, Sofía; Mellado, Virginia & Tascón, Antonio (1992). Medicina tradicional y enfermedad [Traditional Medicine and Illness]. In Roberto Campos (Ed.), La antropología médica en México, Tomo 2. Antologías Universitarias (pp.71-104). México: Instituto Mora, Universidad Autónoma Metropolitana.
Shoshana BERENZON GORN studied her Bachelor's degree in Psychology at the National Autonomous University of Mexico (UNAM) obtaining her degree in 1994. Subsequently studied her Master's and PhD's on Social Psychology at the National Autonomous University of Mexico, obtaining her PhD in 2003. Researcher at the National Institute of Psychiatry in Mexico, working at the Division of Epidemiological and Social Research. Her research interests are drug abuse, mental health, and alternative resources to treat mental health problems. Professor at the National Autonomous University of Mexico. She has published 24 articles in national and international journals, 20 book chapters. She has participated in 42 national and international congresses.
Contact:
Ph D. Shoshana Berenzon Gorn
Division of Epidemiological and Social Research,
National Institute of Psychiatry
Calzada México-Xochimilco 101
Col. San Lorenzo Huipulco
Delegación Tlalpan, C.P. 14370, México, D.F.
E-mail: berenz@imp.edu.mx
Emily ITO SUGIYAMA received her Bachelor's, Master's and Ph.D. in Psychology from the National Autonomous University of Mexico (UNAM). She is currently a full time Tenure Professor of Psychology at UNAM and Chair of the Social Psychology Department. She teaches methodology to undergraduate and graduate students. Her research topics include cultural values, identity and sociopsychological impact of economic globalization.
Contact:
Ph. D. Emily Ito Sugiyama
National Autonomous University of Mexico (UNAM)
Av. Universidad 3004
Col. Copilco-Universidad, C.P. 04510
Del. Coyoacán, México, D.F.
E-mail: emily@servidor.unam.mx
Berenzon Gorn, Shoshana & Sugiyama Ito, Emily (2004). Between Traditional and Scientific Medicine: A Research Strategy for the Study of the Pathways to Treatment Followed by a Group of Mexican Patients with Emotional Disorders [60 paragraphs]. Forum Qualitative Sozialforschung / Forum: Qualitative Social Research, 5(2), Art. 2, http://nbn-resolving.de/urn:nbn:de:0114-fqs040229.

Creative Commons Attribution 4.0 International License